Overview
what it is and why it matters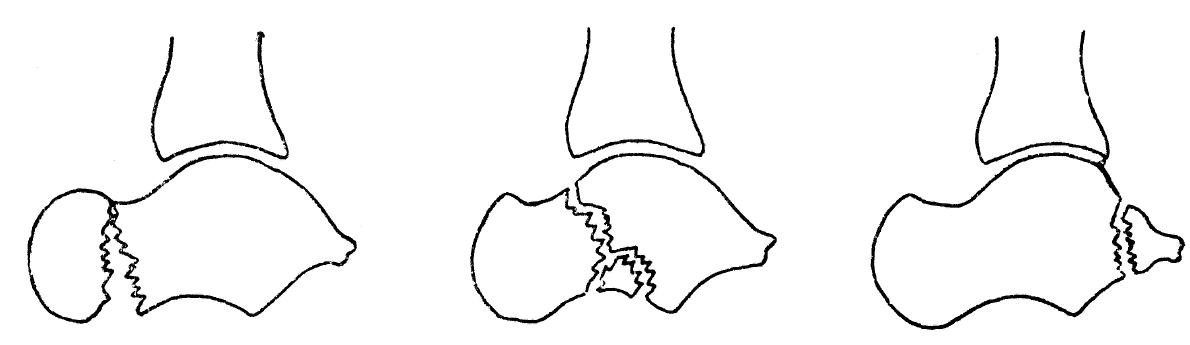
Talar fractures are rare but serious injuries. The talus transmits all body weight between the tibia and the foot and has a precarious blood supply — 60–70% of its surface is covered by articular cartilage, leaving little room for vascular penetration. Talar neck fractures (the most common type) from high-energy dorsiflexion carry a high risk of avascular necrosis (AVN) of the talar body: Hawkins type I (undisplaced, ~0% AVN), type II (subtalar subluxation, ~40% AVN), type III (talar body dislocation, ~90% AVN).
Diagnosis
exam first, imaging secondX-rays including lateral, AP, and Canale views for talar neck. CT is mandatory for surgical planning. MRI evaluates AVN and residual vascularity. Hawkins sign — subchondral lucency of the talar dome on 6-8 week X-ray — is a favorable prognostic sign indicating revascularization.
Treatment Path
how care progresses at OSINon-weight-bearing cast
Hawkins type I undisplaced talar neck fractures may be treated with NWB casting for 8-10 weeks, with close follow-up for displacement or AVN.
Surgical Options at OSI
if non-operative care isn't enoughDisplaced talar neck fractures require urgent anatomic reduction and fixation to minimize AVN risk. Emergency surgery for dislocated talar body fractures.
Further Reading
authoritative sourcesExternal patient-education references and related OSI pages for additional background: