Overview
what it is and why it matters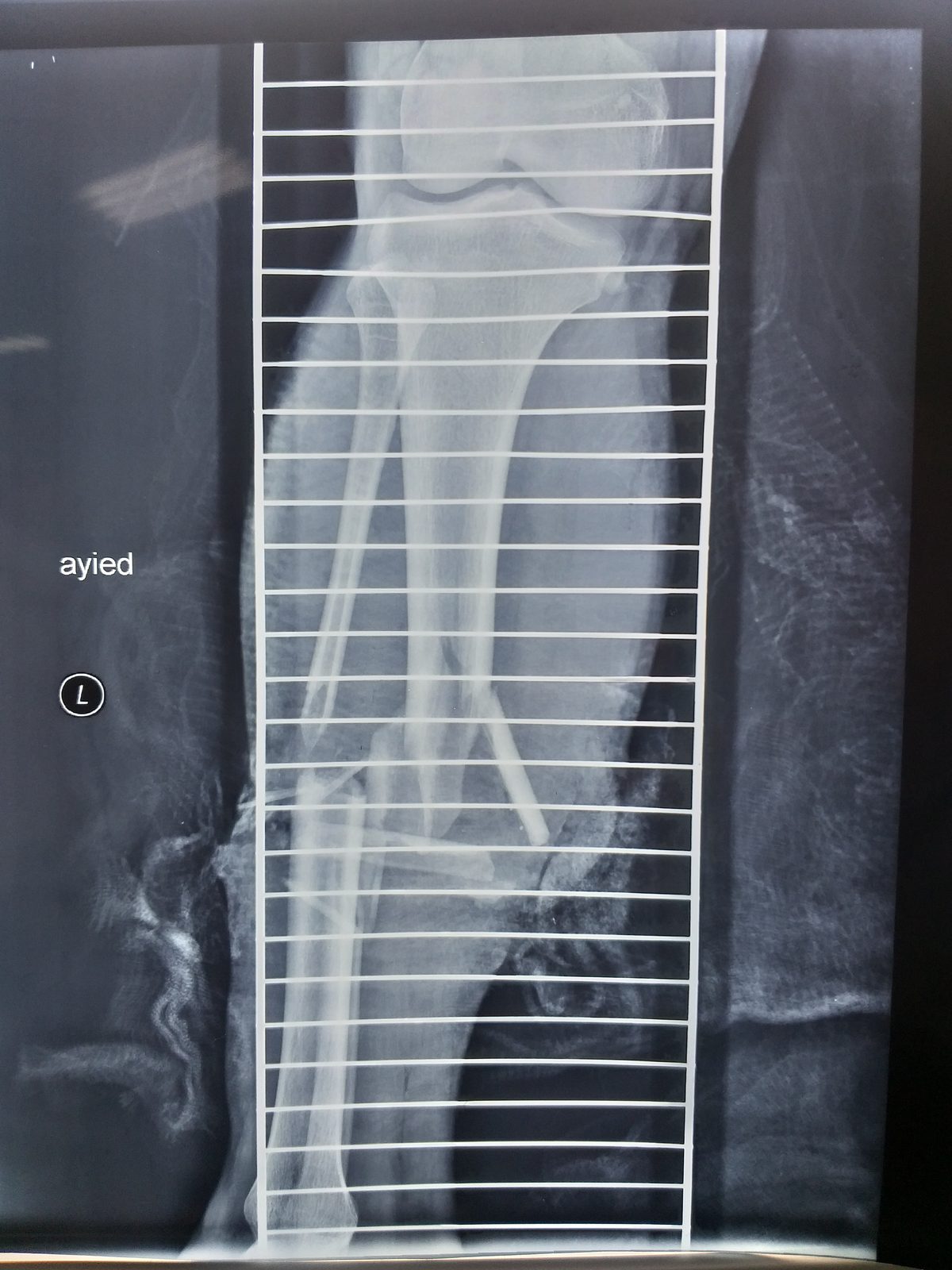
Open (compound) fractures are orthopedic emergencies in which the fracture communicates with the outside environment through a wound, dramatically increasing infection risk — including osteomyelitis and septic arthritis. The Gustilo-Anderson classification (I–IIIC) grades severity by wound size, degree of soft-tissue stripping, vascular injury, and contamination, and guides the aggressiveness of management. IIIB and IIIC injuries with massive soft-tissue loss require plastic surgery collaboration for wound coverage.
Immediate care includes wound coverage with a saline-moistened dressing, antibiotic administration within 1 hour, tetanus prophylaxis, and urgent surgical irrigation and debridement.
Diagnosis
exam first, imaging secondClinical diagnosis. X-rays of the fracture and adjacent joints. CT may be needed for complex fracture characterization. Vascular assessment (ABI, CT angiography) for IIIC injuries with suspected vascular injury.
Treatment Path
how care progresses at OSIWound coverage and antibiotics
Pre-operative management: saline-moistened dressing over the wound, cephalosporin (+ aminoglycoside for grade III, + penicillin for farm/fecal contamination), tetanus prophylaxis.
Surgical Options at OSI
if non-operative care isn't enoughAll open fractures require urgent surgical irrigation and debridement (I&D) — ideally within 6 hours, though recent evidence suggests 24 hours is acceptable for most grade I/II injuries when antibiotics are started promptly.
Further Reading
authoritative sourcesExternal patient-education references and related OSI pages for additional background: