Overview
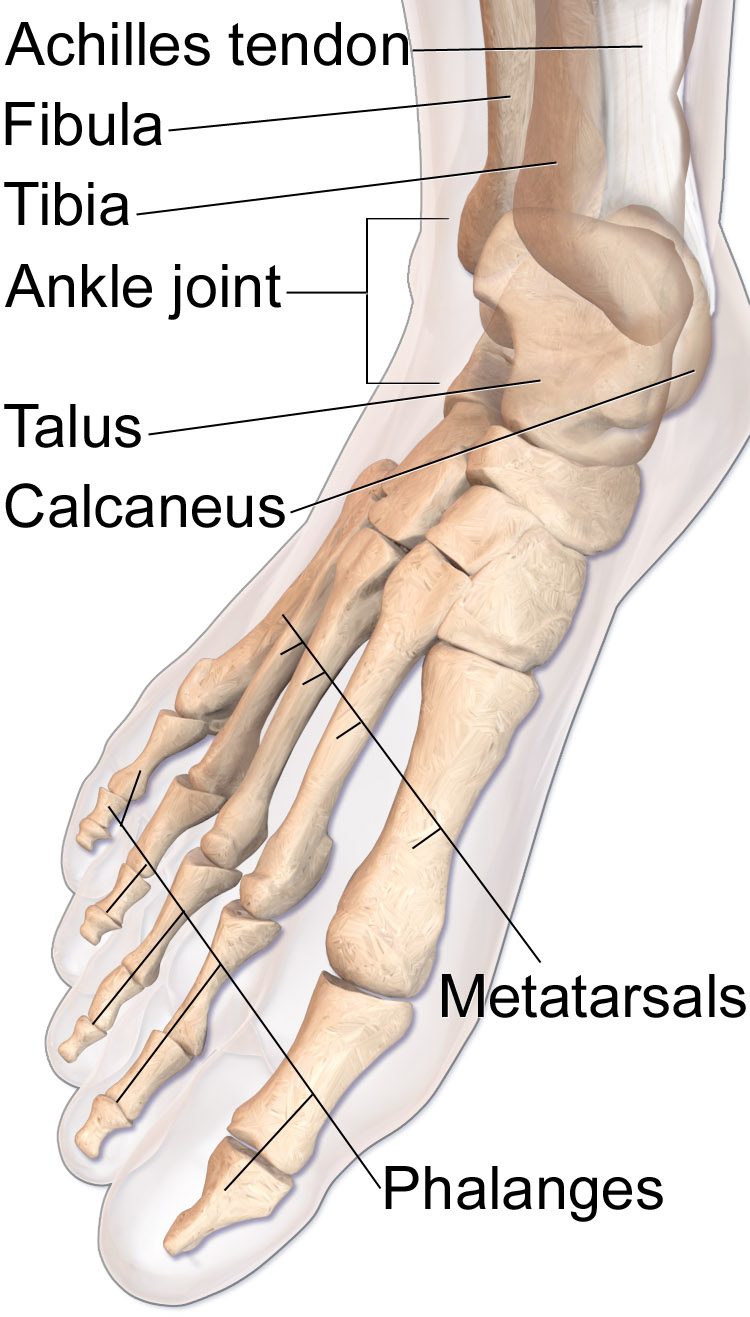
A Jones fracture is a specific break at the base of the fifth metatarsal — the outer bone of the foot — in a watershed blood-supply zone. Because the blood supply is sparse, these fractures are prone to delayed union and nonunion, especially in athletes and in patients with high activity demands.
Operative fixation is often preferred in active patients and athletes who want a quicker, more predictable return to sport. Non-operative treatment with strict non-weight-bearing casting remains an option, particularly in less active patients, but takes longer and carries a higher nonunion risk.
Why it's done
Fifth metatarsal (Jones) ORIF is typically considered when imaging and the clinical picture together indicate that the fracture will not reliably heal or function without surgical stabilization. Common indications include:
Active or athletic patient
A more predictable return to cutting and running sports.
Displaced fracture
Displacement lowers the already-marginal healing rate.
Delayed or nonunion from prior non-operative care
A screw plus biologic augmentation often salvages a stalled fracture.
Chronic stress reaction at the Jones site
Prophylactic fixation may be appropriate in an in-season athlete.
How it works
Through a small incision at the base of the fifth metatarsal, a cannulated solid screw is driven down the medullary canal of the bone under fluoroscopic guidance. The screw compresses the fracture and acts as an internal splint.
In high-risk patients or in nonunion cases, bone graft or biologic augmentation may be added.
Recovery
Patients are typically non-weight-bearing in a boot for two to four weeks, then allowed to progress weight-bearing in the boot. Return to running and cutting activity is usually at twelve weeks once X-rays confirm union. Screws are left unless symptomatic. Re-fracture through or around the screw is a known risk, particularly if the patient returns to sport before full radiographic union.
Contact
For questions about this procedure or to schedule an evaluation, call the office at (830) 625-0009 or request an appointment online.
Further Reading
External patient-education references and related OSI pages for additional background: