Overview
what it is and why it matters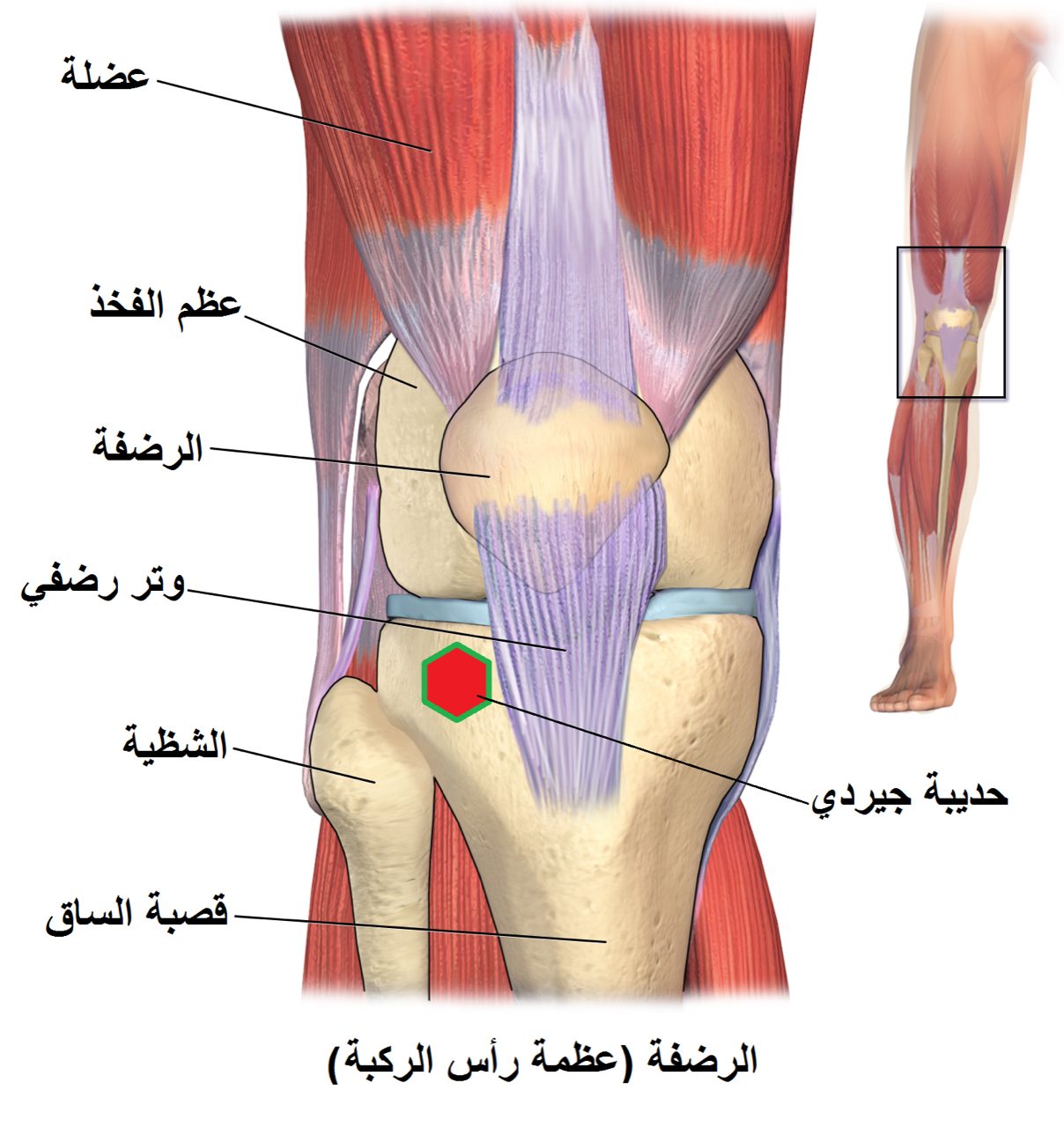
The patellar tendon connects the inferior pole of the patella to the tibial tubercle, completing the extensor mechanism of the knee. Ruptures typically occur in patients under 40 — in contrast to quadriceps ruptures, which tend to occur in older patients. The mechanism is an eccentric quadriceps contraction — a stumble during sport, a hard landing — that overwhelms the tendon. Pre-existing tendinopathy weakens the tendon and predisposes to rupture.
Diagnosis
exam first, imaging secondAcute pain below the kneecap, inability to extend the knee, and a palpable defect below the patella. Lateral X-ray shows a high-riding patella (patella alta). MRI confirms the diagnosis and locates the rupture site (proximal, midsubstance, or distal).
Treatment Path
how care progresses at OSI1
Non-operative management
Not appropriate for complete ruptures — only partial tears with an intact mechanism are managed non-operatively.
Surgical Options at OSI
if non-operative care isn't enoughComplete patellar tendon ruptures require prompt surgical repair. Delay allows the tendon to retract and the extensor mechanism to shorten, making repair more technically difficult.
Providers Who Treat Patellar Tendon Rupture
sports-medicine team

David B. Templin, M.D.

Trent Twitero, M.D.
Further Reading
authoritative sourcesExternal patient-education references and related OSI pages for additional background: