Overview
what it is and why it matters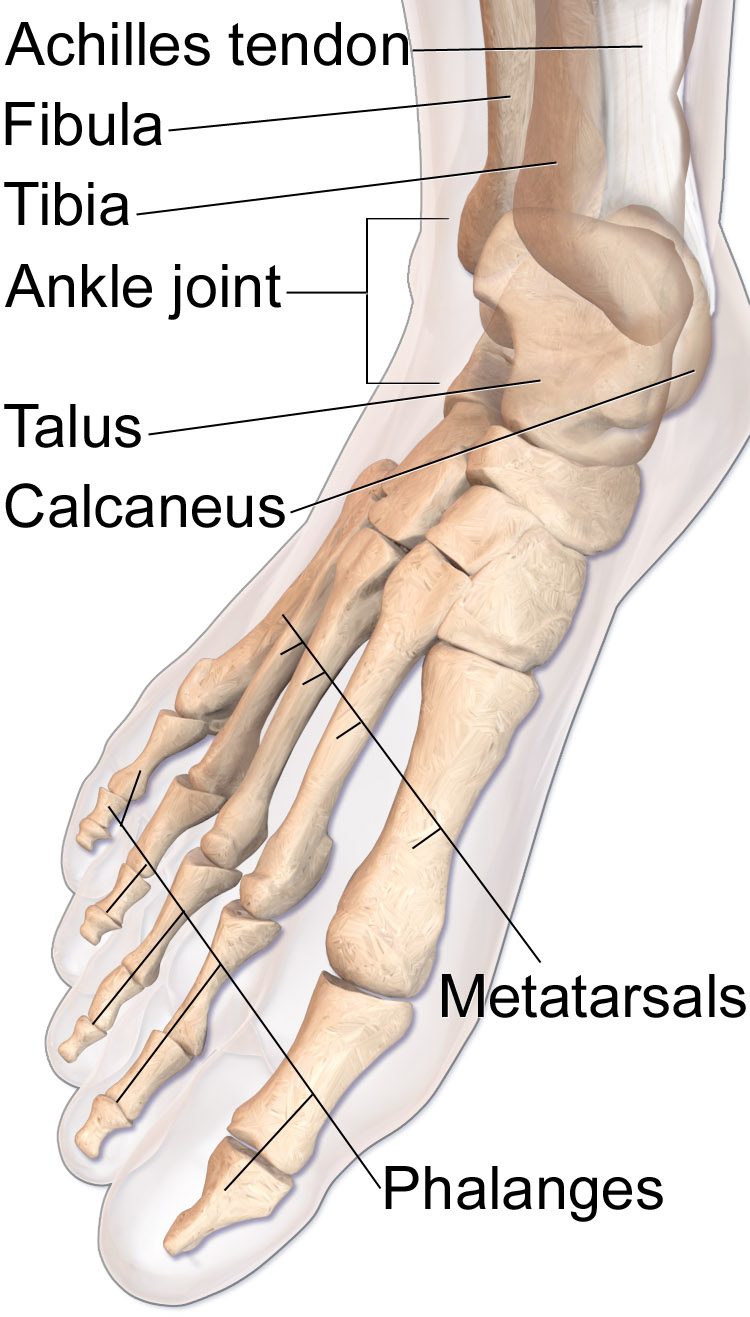
Achilles tendinopathy is a degenerative condition of the Achilles tendon — the largest and strongest tendon in the body — rather than a classic inflammatory "tendinitis." Repetitive overloading causes intratendinous collagen disorganization (tendinosis) at either the mid-portion (2–7 cm above the heel, the "watershed zone" with poorest blood supply) or the insertion at the calcaneus (insertional tendinopathy). Runners are disproportionately affected.
Symptoms include aching posterior heel pain, tendon thickening, and morning stiffness that warms up with activity. A fusiform nodule at the mid-tendon is characteristic of mid-portion tendinopathy.
Diagnosis
exam first, imaging secondClinical diagnosis. The Royal London Hospital test — tenderness at mid-tendon that decreases with passive dorsiflexion — helps distinguish mid-portion from insertional disease. Ultrasound confirms tendon thickening, hypoechoic change (degeneration), and neovascularization. MRI provides better soft-tissue detail for surgical planning.
Treatment Path
how care progresses at OSIEccentric loading protocol (Alfredson)
Eccentric heel drops off a step — the most evidence-backed treatment for mid-portion tendinopathy. 3 sets of 15 reps twice daily for 12 weeks.
Load management
Reducing mileage or intensity while building load tolerance gradually.
Heel lift
Reduces tensile load on the tendon, especially helpful for insertional disease.
Physical therapy
Heavy slow resistance (HSR) program, shockwave therapy adjunct.
Extracorporeal shock wave therapy
Effective for both mid-portion and insertional tendinopathy, particularly in chronic cases.
PRP injection
Evidence supports PRP over corticosteroid (which risks rupture); may be combined with needling/tenotomy.
Surgical Options at OSI
if non-operative care isn't enoughSurgery is considered after 3–6 months of eccentric loading and adjunct therapies have failed.
Further Reading
authoritative sourcesExternal patient-education references and related OSI pages for additional background: