Overview
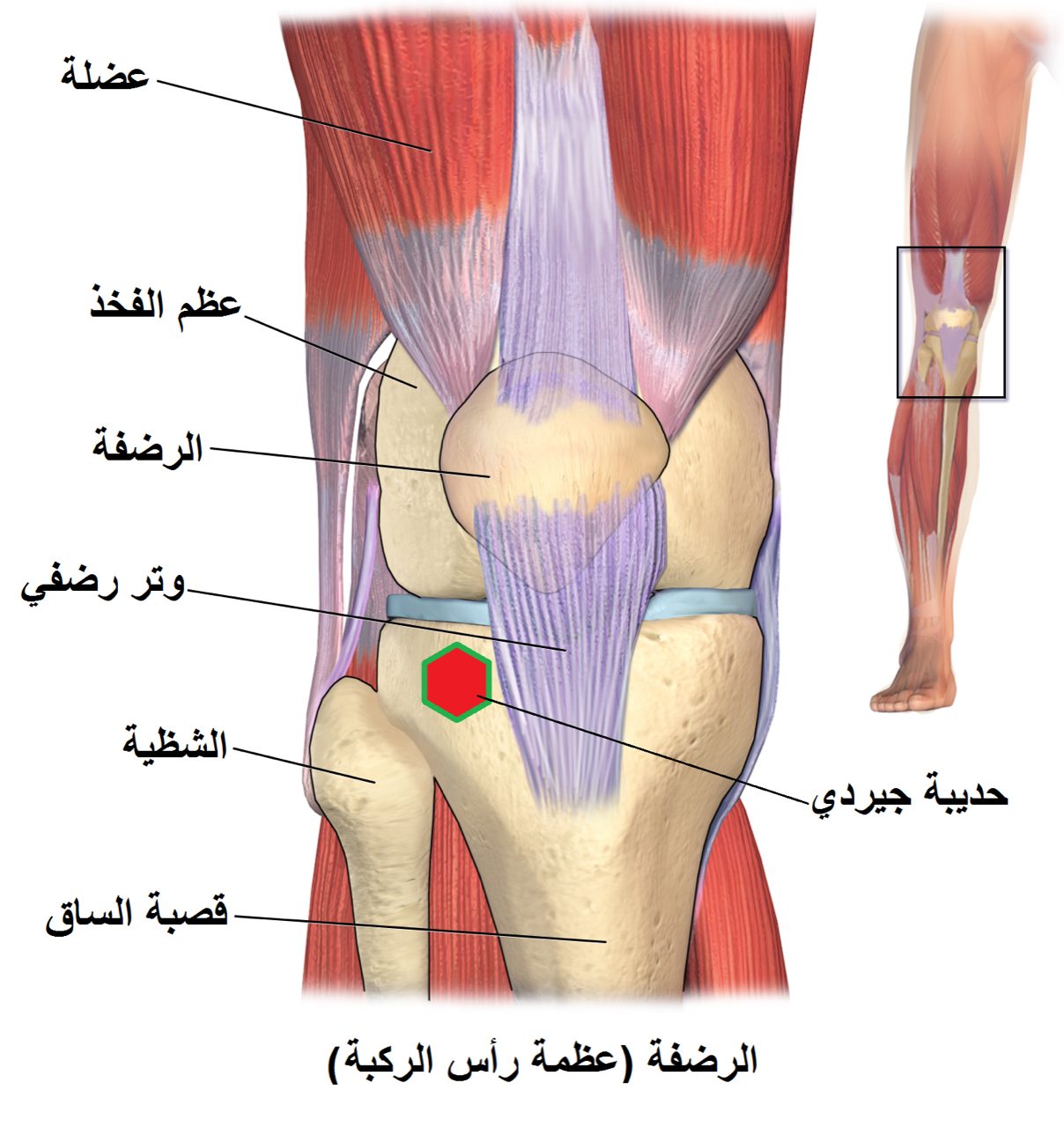
The patella is the kneecap — a sesamoid bone embedded in the quadriceps and patellar tendons. A displaced patella fracture disconnects the mechanism that straightens the knee, which makes it impossible to actively extend the leg against gravity.
Operative fixation is indicated for displaced fractures, any fracture with loss of active extension, and most comminuted patterns. Non-displaced fractures with an intact extensor mechanism can usually be treated in a brace.
Why it's done
Patella ORIF is typically considered when imaging and the clinical picture together indicate that the fracture will not reliably heal or function without surgical stabilization. Common indications include:
Loss of active knee extension
The key clinical indication for surgery.
Displacement greater than about 3 mm
Displacement continues under quadriceps pull.
Articular step-off
The back of the patella is a joint surface.
Open fracture
Urgent debridement and fixation.
How it works
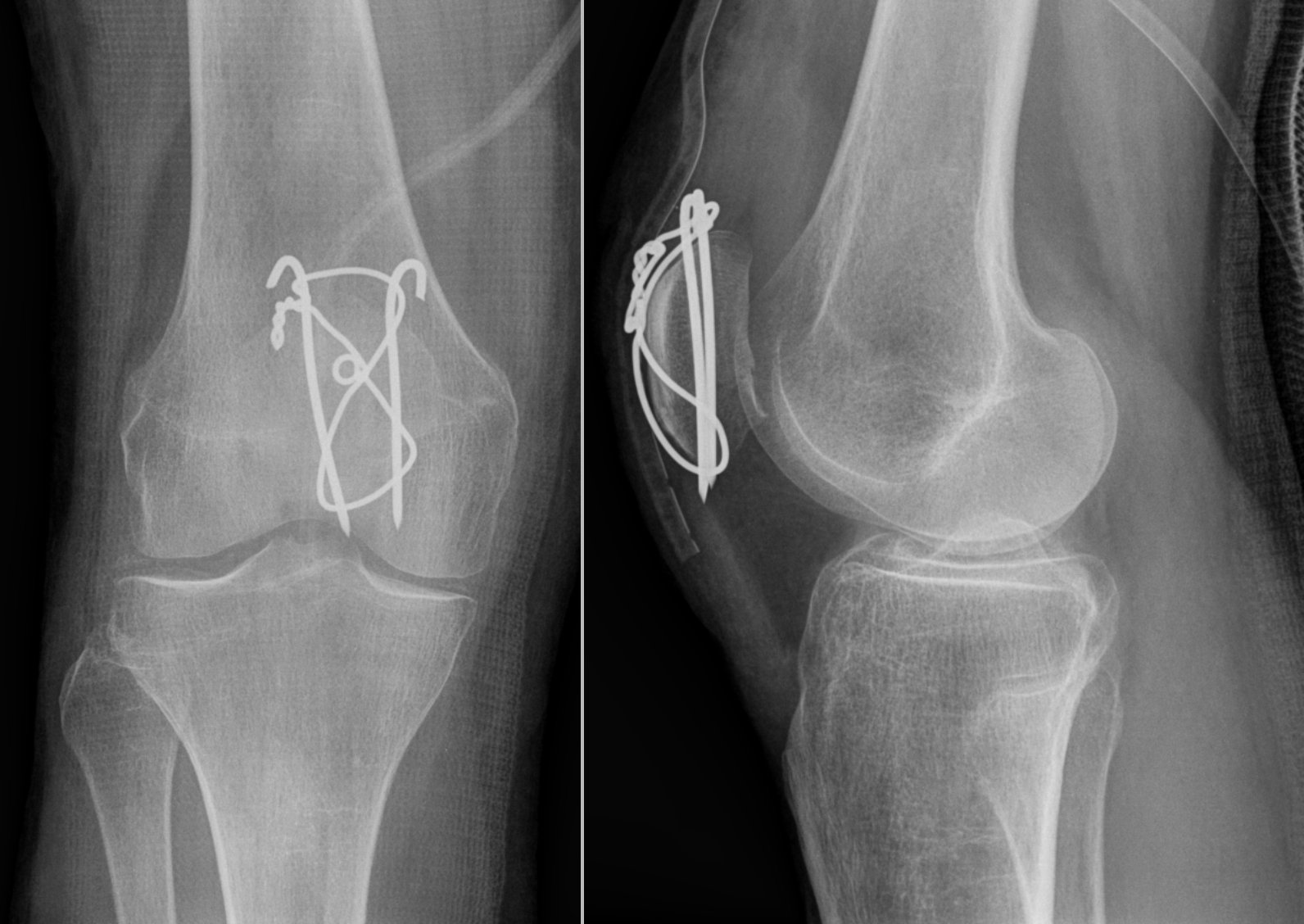
Simple transverse fractures are typically fixed with two cannulated screws and a figure-of-eight suture or wire tension band. This converts the pull of the quadriceps into compression across the fracture.
Comminuted fractures are fixed with a combination of screws, plates, and cerclage constructs through an anterior midline incision. The goal is a congruent articular surface on the back of the patella.
Recovery
The knee is protected in a brace locked in extension for walking during the first four to six weeks. Toe-touch or protected weight-bearing is used initially. Passive and active-assisted knee flexion begins early to prevent stiffness. Active extension against resistance is delayed until the fracture is healed. Full recovery takes three to six months. Hardware irritation is common and removal is sometimes needed later.
Contact
For questions about this procedure or to schedule an evaluation, call the office at (830) 625-0009 or request an appointment online.
Further Reading
External patient-education references and related OSI pages for additional background: