Overview
what it is and why it matters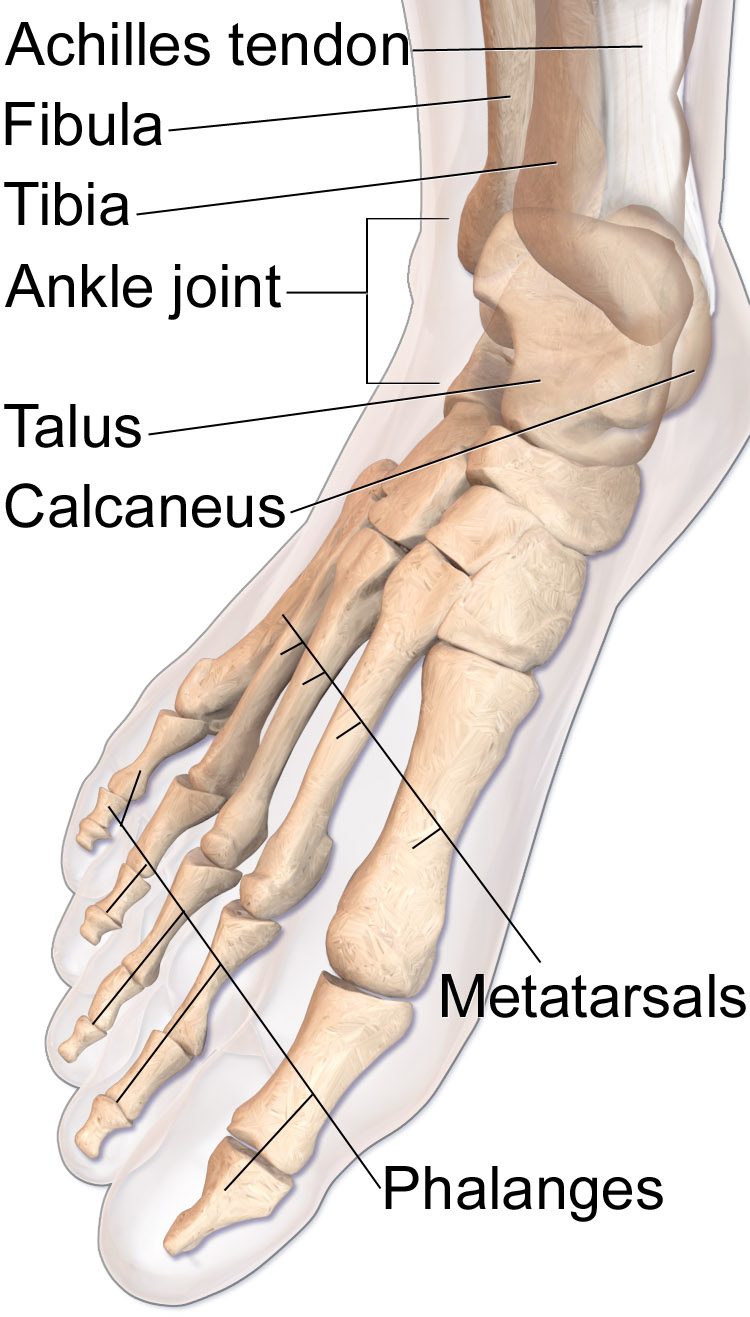
Achilles tendon rupture is a complete disruption of the tendon, most commonly occurring 2–6 cm proximal to the calcaneal insertion in the relatively avascular mid-substance. The classic mechanism is a sudden forceful plantarflexion — pushing off to sprint, jumping, or stepping into a pothole — often described as feeling like being kicked in the back of the leg. Most patients report a loud "pop."
Rupture is most common in the "weekend warrior" — deconditioned men in their 30s–50s who engage in sudden bursts of activity. Prior steroid injections and fluoroquinolone antibiotics are risk factors.
Diagnosis
exam first, imaging secondThe Thompson test is the key exam: with the patient prone and knees bent, squeezing the calf should plantarflex the foot — absence of plantarflexion confirms a complete rupture. A palpable gap above the heel and inability to perform a single-leg heel rise support the diagnosis. Ultrasound confirms the rupture and gap size. MRI is used preoperatively for complex cases.
Treatment Path
how care progresses at OSIFunctional rehabilitation protocol (non-operative)
Serial casting in plantarflexion followed by a functional brace with progressive dorsiflexion allows end-to-end healing without surgery. Modern studies show re-rupture rates equivalent to surgery in properly selected patients when an accelerated functional protocol is used.
Surgical Options at OSI
if non-operative care isn't enoughOperative repair is preferred in young, active, and athletic patients who want the fastest reliable return to sport. Non-operative treatment is a reasonable alternative for lower-demand patients or those with medical contraindications to surgery.
Further Reading
authoritative sourcesExternal patient-education references and related OSI pages for additional background: