Overview
When a younger, active patient has arthritis limited to one side of the knee — usually medial — and their leg bows into varus, the damaged compartment is overloaded with every step. Replacing the knee would work, but a joint replacement has a finite lifespan in a demanding patient. Realigning the tibia shifts load off the worn compartment and preserves the native joint.
How the Procedure Works
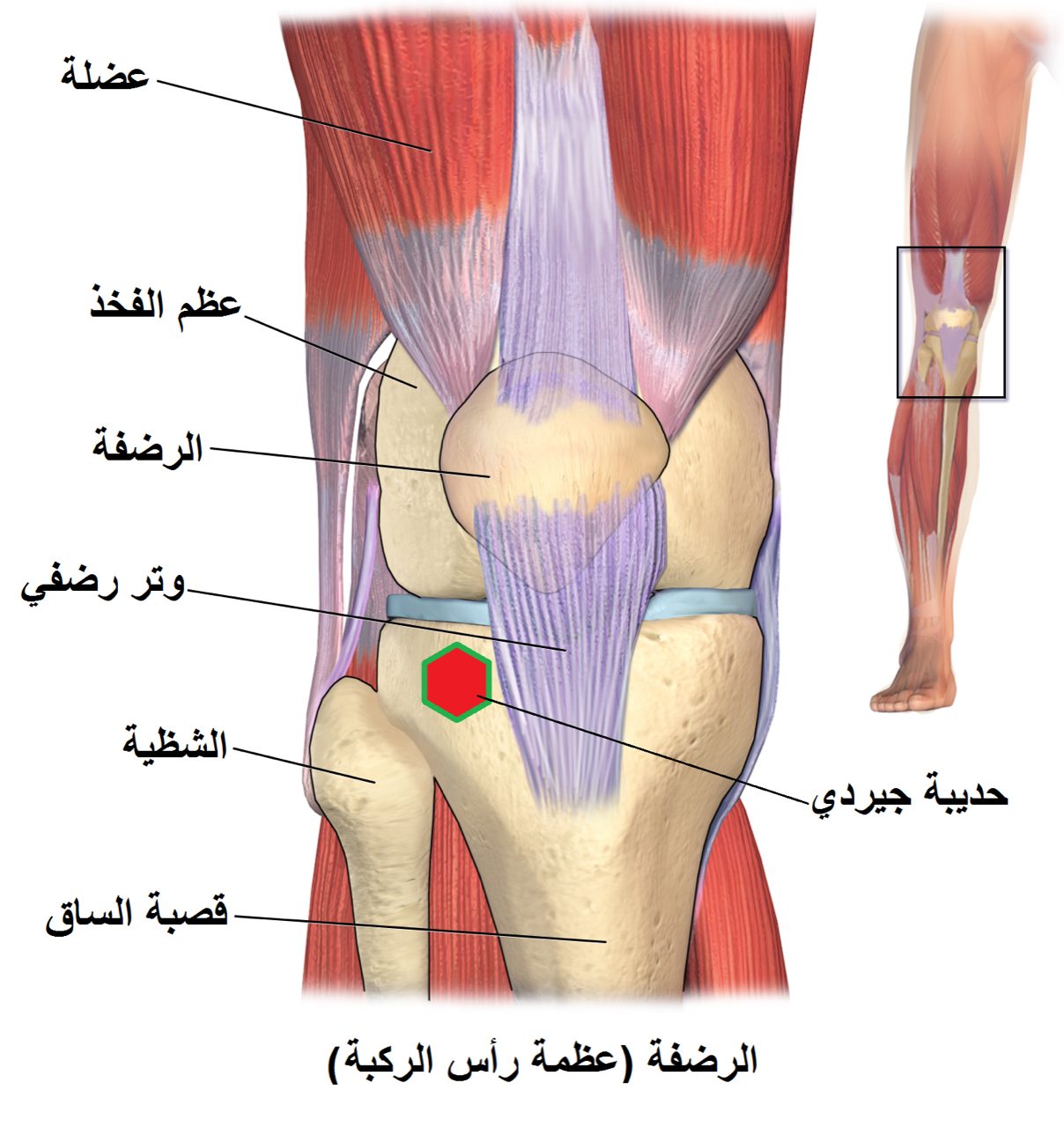
The correction angle is calculated preoperatively from standing long-leg X-rays — we aim to shift the mechanical axis from the worn compartment to a point just lateral to the center of the joint, typically to 62–66% across the tibial plateau. Under-correction leaves the patient with residual pain; over-correction unloads the repaired compartment but overloads the opposite one. We use a medial opening-wedge technique in most cases: a transverse cut is made in the proximal tibia, the wedge is opened to the planned angle under fluoroscopy, filled with bone graft or substitute, and held with a locking plate. The lateral cortex is left partially intact as a hinge — maintaining that hinge prevents the osteotomy from collapsing before it heals. Patients are protected with partial weight-bearing for six to eight weeks while the bone consolidates.
When to Consider High Tibial Osteotomy
High tibial osteotomy is generally offered when symptoms, imaging, and a trial of non-operative care together point to surgery as the next step. The typical picture includes:
Unicompartmental arthritis with malalignment
Isolated medial or lateral compartment wear, matched to a varus or valgus leg axis on standing X-rays.
Active patient preserving a native knee
Patients who want to keep running, hiking, or doing physical work that would stress a knee replacement.
Preserved motion and ligaments
A knee with good range of motion and intact cruciate and collateral ligaments.
Conditions This Treats
Physicians Who Perform High Tibial Osteotomy


David B. Templin, M.D.

Trent Twitero, M.D.
Providers Who Surgically Assist with High Tibial Osteotomy

Sydney Georg, PA-C
Ben Swanner, PA-C
Further Reading
External patient-education references and related OSI pages for additional background: