Overview

When a shoulder has dislocated repeatedly, the anterior glenoid rim erodes. Once bone loss is significant, a soft-tissue Bankart repair will fail. The Latarjet procedure addresses the problem both structurally and dynamically: a piece of the coracoid process, with its conjoint tendon still attached, is transferred to the front of the glenoid.
How the Procedure Works
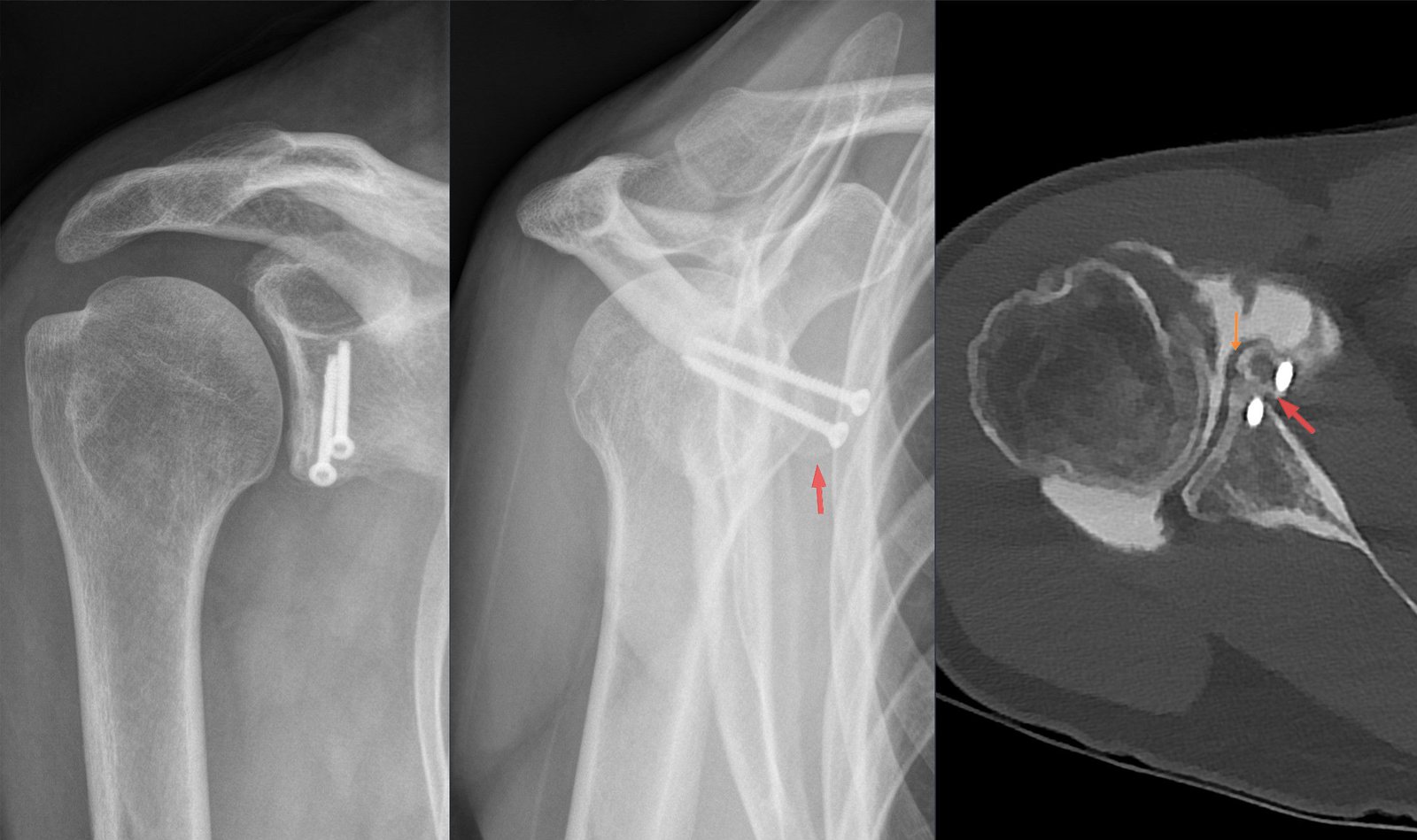
We split the subscapularis horizontally — rather than detach it — to pass the coracoid through to the front of the glenoid while keeping the muscle's function intact. The coracoid is positioned flush with the glenoid face, not proud: a block that stands too high impinges on the humeral head, too low fails to extend the arc. Two screws fix the bone block; their direction and purchase in the glenoid neck determine whether it stays put under load. The conjoint tendon crossing the subscapularis contributes a second layer of protection — it tightens when the arm moves into abduction and external rotation, which is exactly the position that used to dislocate the shoulder. The musculocutaneous nerve runs immediately medial to the coracoid during harvest, and the axillary nerve lies at the inferior border of the subscapularis split; both are identified and protected throughout.
When to Consider Latarjet Procedure
Latarjet procedure is generally offered when symptoms, imaging, and a trial of non-operative care together point to surgery as the next step. The typical picture includes:
Recurrent dislocation after Bankart repair
A shoulder that continues to dislocate despite prior soft-tissue stabilization.
Significant anterior glenoid bone loss
Bone loss that exceeds the threshold at which a Bankart repair alone is predictably durable.
High re-dislocation risk
Contact athletes whose sport profile makes even a small recurrence risk unacceptable.
Conditions This Treats
Physicians Who Perform Latarjet Procedure


David B. Templin, M.D.

Trent Twitero, M.D.
Providers Who Surgically Assist with Latarjet Procedure

Sydney Georg, PA-C
Ben Swanner, PA-C
Further Reading
External patient-education references and related OSI pages for additional background: