Overview
what it is and why it matters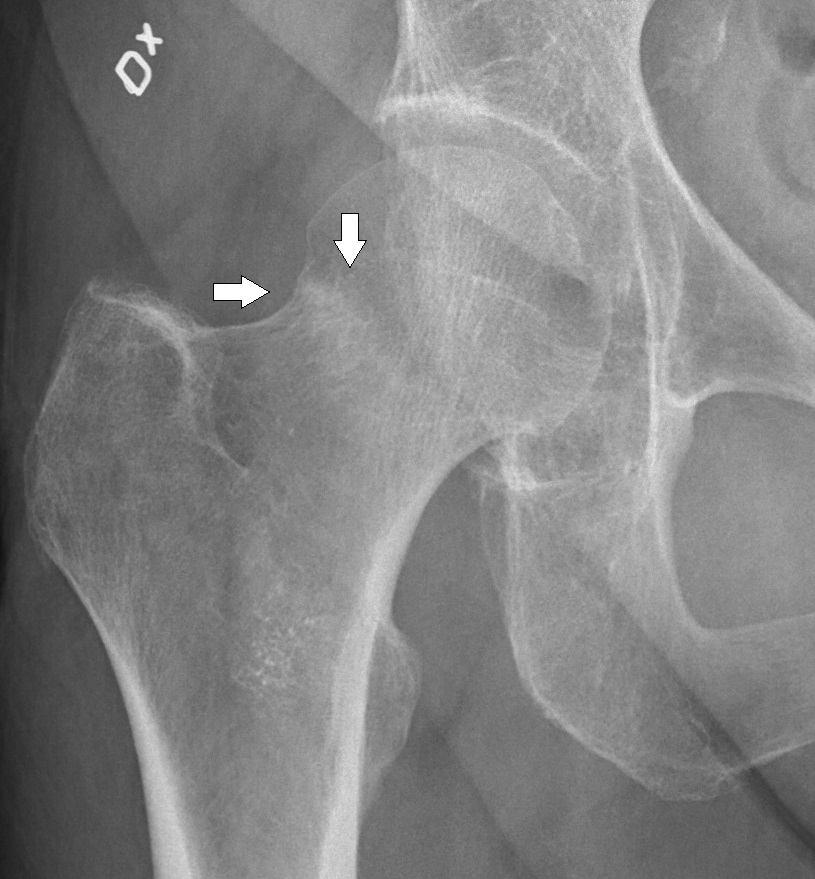
The femoral neck is the angled segment connecting the femoral head (ball) to the shaft of the femur. Fractures here are among the most common and serious orthopedic injuries — particularly in older adults with osteoporosis, where a low-energy fall can break a weakened neck, and in young active patients, where high-energy trauma or repetitive stress can fracture an otherwise normal bone.
Femoral neck fractures in older adults are associated with significant morbidity and mortality; up to 20–30% of elderly patients die within one year of injury. Early surgical fixation or replacement — ideally within 24–48 hours — is the standard of care because prolonged bed rest carries higher risks than surgery.
Diagnosis
exam first, imaging secondDisplaced fractures present with inability to bear weight, a shortened and externally rotated leg, and groin pain. Nondisplaced fractures may present with groin pain only. AP pelvis and lateral hip X-rays confirm most fractures. CT or MRI is used for suspected non-displaced or stress fractures not seen on X-ray.
Treatment Path
how care progresses at OSI1
Non-operative management
Reserved for non-displaced stable fractures in carefully selected patients who are not surgical candidates due to severe medical comorbidities. Protected weight-bearing and close follow-up are required.
Surgical Options at OSI
if non-operative care isn't enoughThe large majority of femoral neck fractures require surgery. The choice between fixation and replacement depends on the degree of displacement, the patient's age and bone quality, and the integrity of the blood supply to the femoral head.
Providers Who Treat Femoral Neck Fracture
sports-medicine team

David B. Templin, M.D.

Trent Twitero, M.D.
Further Reading
authoritative sourcesExternal patient-education references and related OSI pages for additional background: