Overview
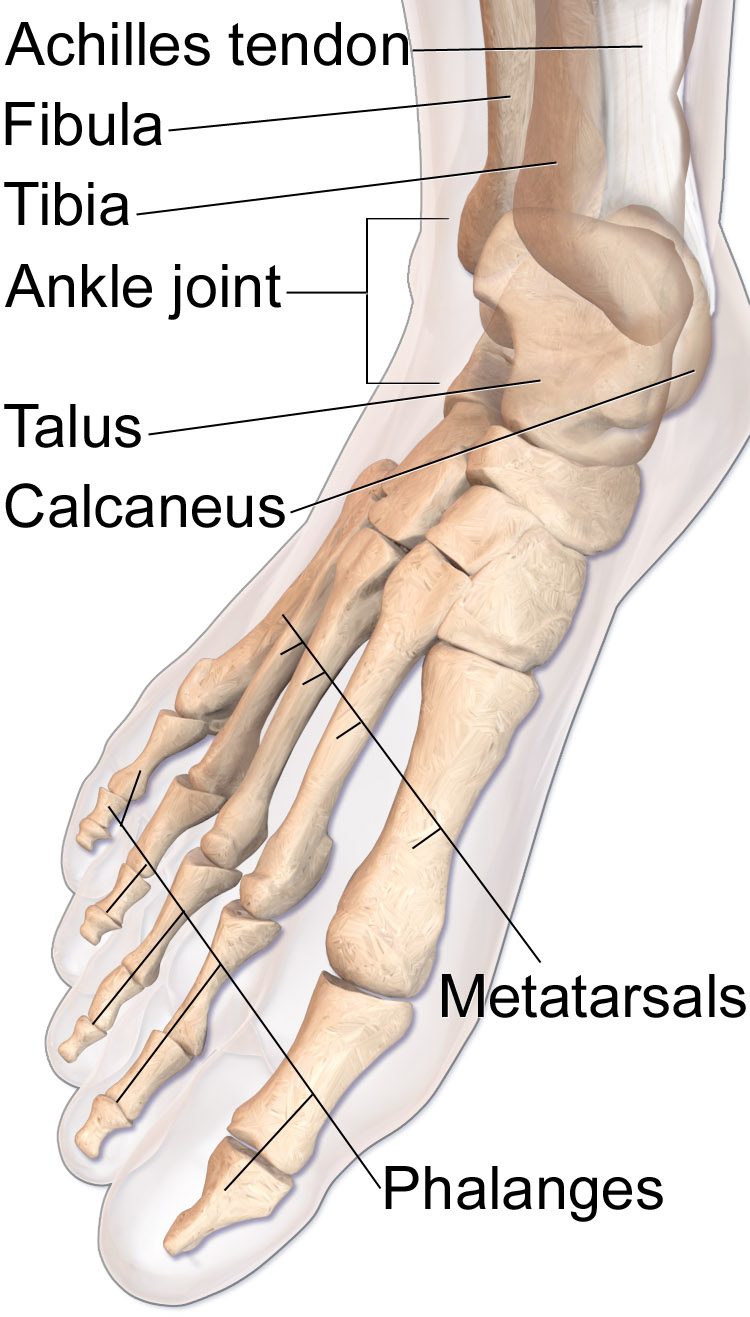
The talus is the central bone of the hindfoot and articulates with the tibia above, the calcaneus below, and the navicular in front. It has a precarious blood supply and no direct muscular attachments. Displaced talus fractures carry a high risk of avascular necrosis and post-traumatic arthritis.
Operative fixation is indicated for essentially all displaced fractures and is typically performed urgently to minimize the risk of skin compromise and to protect the remaining blood supply to the talar body.
Why it's done
Talus fracture fixation is typically considered when imaging and the clinical picture together indicate that the fracture will not reliably heal or function without surgical stabilization. Common indications include:
Displaced talar neck or body fracture
Restoring alignment protects the blood supply.
Subtalar, ankle, or talonavicular joint subluxation or dislocation
Urgent reduction is required.
Open fracture
Immediate debridement and stabilization.
Lateral process fracture with displacement
Often mistaken for an ankle sprain; warrants fixation when displaced.
How it works

Dual anteromedial and anterolateral incisions typically give the needed exposure while preserving skin bridges. The fracture is reduced and fixed with small screws, and a mini-plate is added along the medial or lateral column for comminuted patterns.
For severely displaced patterns, an associated medial malleolar osteotomy is sometimes needed to visualize the joint surface. Fluoroscopy and direct inspection confirm anatomic reduction.
Recovery
Strict non-weight-bearing for ten to twelve weeks is typical. Early ankle and subtalar motion are encouraged once the wound is stable. Serial X-rays monitor for the Hawkins sign — subchondral radiolucency indicating preserved blood supply — at six to eight weeks. Avascular necrosis, subtalar stiffness, and post-traumatic arthritis are known long-term complications. Later subtalar or ankle fusion may be considered if arthritis becomes symptomatic.
Contact
For questions about this procedure or to schedule an evaluation, call the office at (830) 625-0009 or request an appointment online.
Further Reading
External patient-education references and related OSI pages for additional background: