Overview

The clavicle is the strut that holds the shoulder out from the chest wall. Most clavicle fractures occur in the middle third of the bone after a direct fall onto the shoulder. Many heal well in a sling, but fractures that are significantly shortened, displaced, or comminuted have a higher rate of nonunion and poor shoulder function when treated non-operatively.
Surgery is typically offered for shortening greater than about two centimeters, wide displacement, skin tenting, open injury, or certain fracture patterns in active patients who want the most reliable return to full strength.
Why it's done
Clavicle ORIF is typically considered when imaging and the clinical picture together indicate that the fracture will not reliably heal or function without surgical stabilization. Common indications include:
Displacement greater than one bone width
Non-operative healing rates fall sharply with this degree of displacement.
Significant shortening (>2 cm)
Shoulder mechanics and scapular position are altered.
Skin tenting or open fracture
At-risk skin requires reduction and fixation.
Floating shoulder or neurovascular injury
Associated injuries often demand stabilization.
Active patient with functional demands
Plating offers a more predictable return to overhead and throwing activity.
How it works
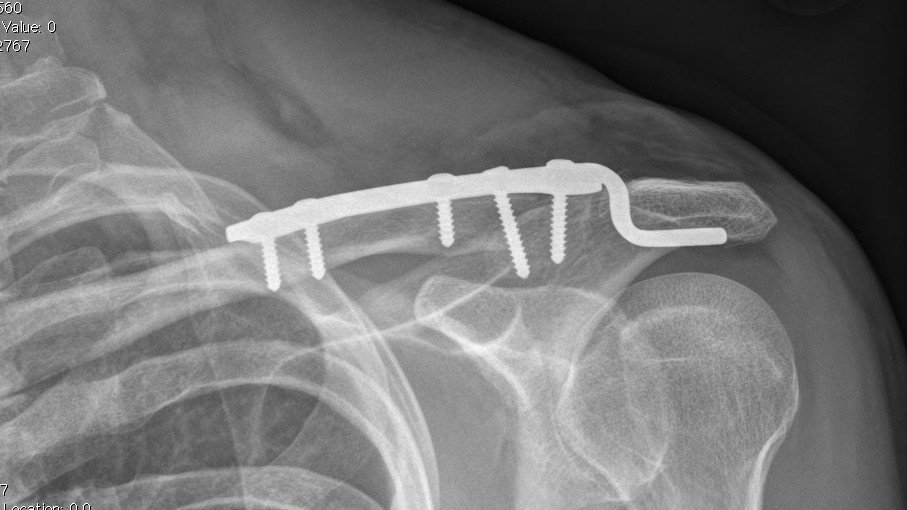
Through an incision along the top or front edge of the clavicle, the fracture is reduced to restore length and rotation. A pre-contoured plate is laid on the bone — either superior or anterior — and secured with multiple screws on each side of the fracture.
Comminuted fragments are typically held in place with small lag screws or sutures. Fluoroscopy confirms reduction and screw length.
Recovery
The arm is kept in a sling for a few weeks, with pendulum and gentle passive motion starting right away. Active motion progresses as pain allows, with return to full overhead use around six to eight weeks. Union is typically confirmed on X-ray by three months. Hardware irritation at the plate is not uncommon; elective hardware removal can be considered once the fracture is fully healed.
Contact
For questions about this procedure or to schedule an evaluation, call the office at (830) 625-0009 or request an appointment online.
Further Reading
External patient-education references and related OSI pages for additional background: