Overview
what it is and why it matters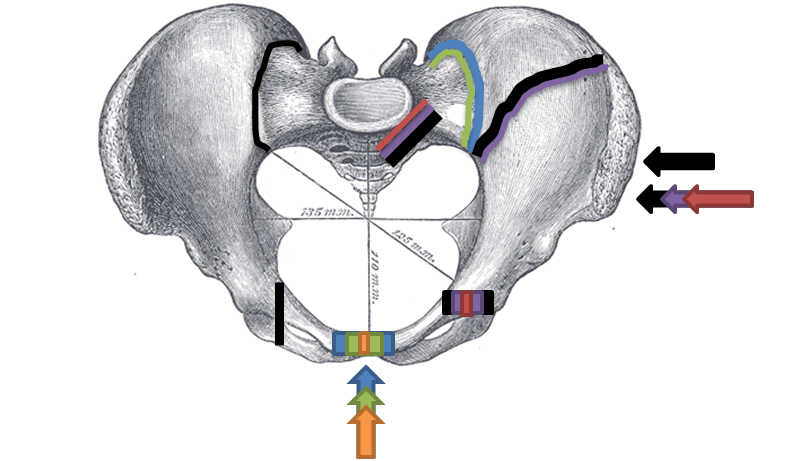
The pelvic ring is formed by the sacrum posteriorly and the two innominate bones (ilium, ischium, pubis) anteriorly, connected at the pubic symphysis and two sacroiliac joints. Fractures range from low-energy avulsion injuries in young athletes and insufficiency fractures in osteoporotic bone, to high-energy ring disruptions from falls from height or sports collisions that cause massive hemorrhage and life-threatening instability.
Tile's AO/OTA classification categorizes pelvic fractures by stability: Type A (stable, minor injury), Type B (rotationally unstable), and Type C (rotationally and vertically unstable). Unstable patterns are orthopedic emergencies.
Diagnosis
exam first, imaging secondLow-energy fractures present with groin or pelvic pain and difficulty bearing weight. High-energy injuries present with hemodynamic instability, obvious deformity, or inability to transfer. AP pelvis X-ray is the primary screening study; inlet and outlet views add information. CT with contrast characterizes the injury pattern and detects vascular injury.
Treatment Path
how care progresses at OSI1
Protected weight-bearing
Appropriate for stable Type A fractures — pelvic rest, analgesia, and gradual return to weight-bearing as tolerated.
Surgical Options at OSI
if non-operative care isn't enoughRotationally or vertically unstable fractures require stabilization. Emergent stabilization may be needed for hemorrhage control before definitive fixation.
Providers Who Treat Pelvic Ring Fracture
sports-medicine team

David B. Templin, M.D.

Trent Twitero, M.D.
Further Reading
authoritative sourcesExternal patient-education references and related OSI pages for additional background: