Overview
what it is and why it matters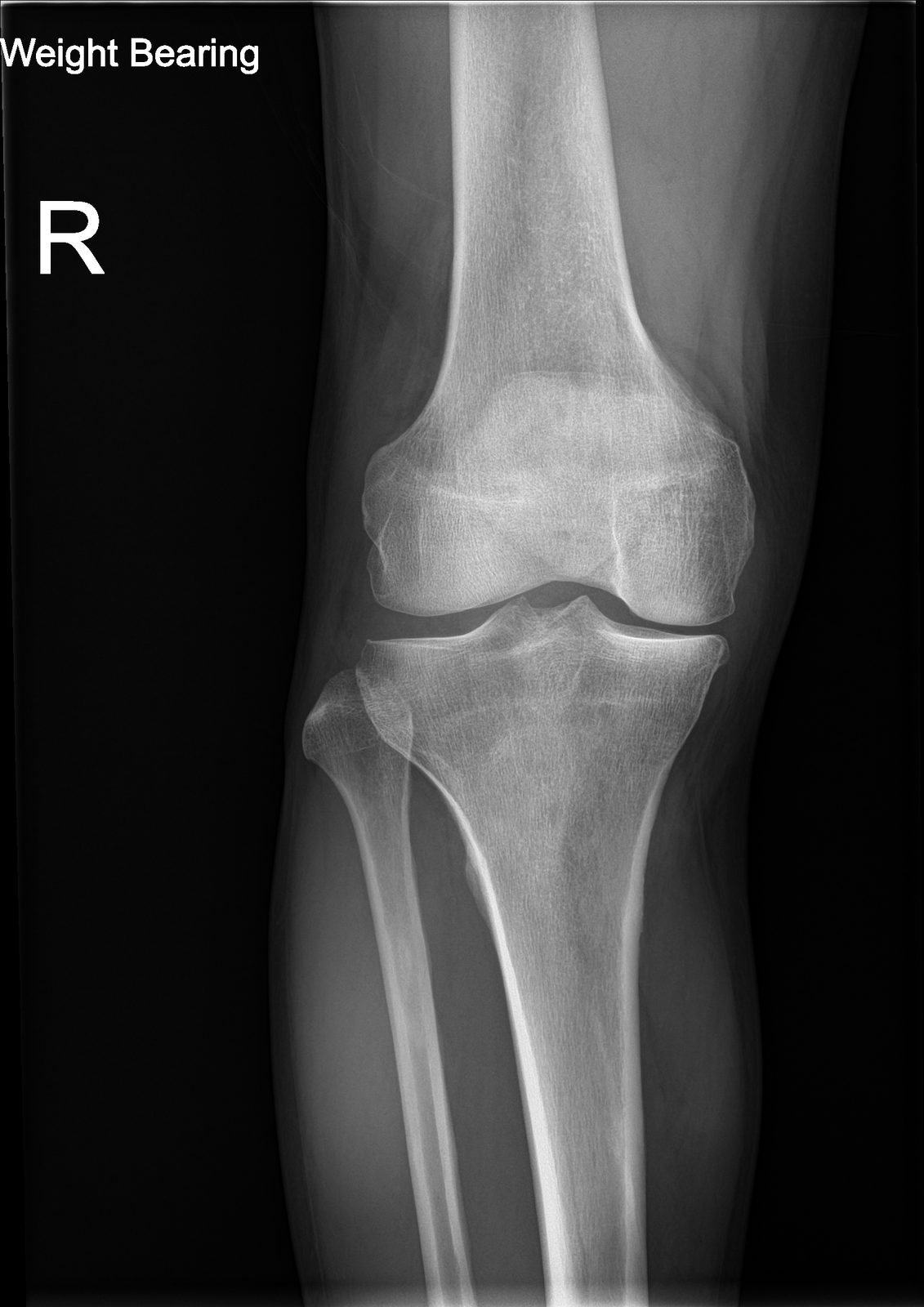
Knee osteoarthritis is the slow wearing-out of the smooth cartilage that lines the three compartments of the knee — the medial (inner) side, the lateral (outer) side, and the patellofemoral joint behind the kneecap. Cartilage cannot feel pain, but the bone underneath it can. Once the cartilage has thinned past a critical point, the bones begin to rub, the body reacts with inflammation, the joint lining thickens, and the edges of the bone grow small outcroppings called osteophytes. The practical result is the kind of knee pain patients describe as "achy and stiff" — worse with stairs, worse after sitting, worse at the end of the day.
Most knee osteoarthritis is primary — the cumulative result of decades of use, genetics, and body weight. Secondary osteoarthritis follows a specific earlier event: a meniscus tear, an ACL rupture, a fracture that entered the joint, or a leg that has always tracked slightly bowed or knock-kneed. Every pound of body weight translates to three or four pounds of force across the knee while walking, which is why weight and cartilage health are tightly linked.
Anatomy & Mechanism
why the knee wearsThe tibiofemoral joint transmits 3–4× body weight during level walking and up to 6× body weight on stairs. Articular cartilage distributes that load; the menisci add shock absorption and joint stability. When cartilage thins, load concentrates, the joint becomes inflamed, and the body lays down osteophytes in an attempt to stabilize itself. Because the medial compartment carries more load than the lateral in most knees, it wears first — which is why many patients with knee OA become progressively bow-legged. Loss of the meniscus through degeneration or prior partial meniscectomy accelerates cartilage loss in that compartment.
Symptoms
what patients describe- Activity-related pain — worse with stairs, inclines, squatting, and rising from a chair
- Morning stiffness lasting under 30 minutes, recurring after prolonged sitting
- Recurrent swelling and a sense of warmth around the joint after activity
- Catching or giving way, particularly when a degenerative meniscus tear coexists
- Night pain and a loss of deep flexion (difficulty kneeling, squatting, or sitting cross-legged) as disease advances
Diagnosis
exam first, imaging secondWeight-bearing X-rays are the imaging standard — a standing anteroposterior, a lateral, and a patellofemoral view (sunrise or Merchant). Non-weight-bearing films routinely underestimate joint-space narrowing because the cartilage is not being compressed by body weight. Radiographic severity is graded on the Kellgren-Lawrence scale (0–4).
MRI is not required to diagnose OA and is reserved for targeted questions — a mechanical meniscus tear in a younger patient, suspicion of osteonecrosis, or soft-tissue pathology that would not show on radiograph. Laboratory testing is limited to cases where inflammatory or crystalline disease is suspected.
Nonoperative Treatment
first line for most patientsThe first goal of treatment is to make the joint comfortable enough to keep using it. Most patients improve meaningfully with a combination of weight management, strengthening, and staged pain control — no injection, no surgery required.
1
Weight management & low-impact conditioning
Every pound lost takes roughly three to four pounds of load off each knee. Cycling, swimming, and elliptical work preserve cardiovascular fitness without concentrating force on the joint.
2
Physical therapy
Strong quadriceps — especially the inner portion that attaches near the kneecap — act as a shock absorber at heel strike and reduce the force the cartilage has to absorb. Hip and core strengthening round out the program.
3
Oral and topical analgesics
Anti-inflammatory medications (ibuprofen, naproxen, meloxicam) provide meaningful pain relief when used intermittently and when heart, stomach, and kidney health allow. Topical diclofenac applied to the skin over the knee is a good alternative when oral anti-inflammatories are not a safe option.
Cortisone injection
An intra-articular corticosteroid injection provides weeks to several months of relief in the right patient and is useful as a bridge to therapy gains or a planned surgery. Repeated frequent injections are avoided.
Hyaluronic acid (viscosupplementation)
Hyaluronic acid is a lubricating fluid injection and has its strongest evidence in the knee. It is a reasonable option for patients who want to delay a knee replacement.
Unloader bracing
An unloader brace uses a three-point bending mechanism to redirect force away from the worn compartment. Patient selection matters — it works best when only the medial or only the lateral side is arthritic and the ligaments are intact.
Biologic injections (PRP)
Platelet-rich plasma is prepared from your own blood and injected into the joint. It has shown promise in mild-to-moderate osteoarthritis and is considered after standard options have been tried. PRP is not covered by insurance and is offered at a flat self-pay rate.
Operative Treatment
when function no longer respondsThe decision to operate is rarely driven by the X-ray alone — it rests on how much the knee is interfering with life. Surgery is considered when nonoperative care no longer provides adequate relief, when pain is waking you at night, when activities that matter are being avoided, or when daily pain medication has become necessary to function. Modern total knee replacement is one of the most successful operations in medicine, with more than 95% of implants still in place and working well a decade after surgery.
Primary procedure
Total knee replacement
Resurfacing of all three knee compartments. The standard operation for end-stage tricompartmental or advanced bicompartmental disease.
Learn about this procedure →Additional option
Partial (unicompartmental) knee replacement
For isolated medial or lateral compartment disease with intact ligaments — resurfaces only the worn compartment, preserves native anatomy, and offers a faster recovery.
Learn about this procedure →Additional option
High tibial osteotomy
Realignment procedure that unloads the worn compartment in younger, active patients with varus malalignment and unicompartmental disease.
Learn about this procedure →Recovery & Expectations
what care looks like after surgeryRecovery after knee replacement moves through predictable phases, but the pace is individual. Early rehabilitation focuses on swelling control, quadriceps activation, and restoring range of motion. Strengthening progresses as healing permits, and walking distance and gait quality become the benchmarks for weaning any assistive device. The final phase is a gradual return to everyday activity and low-impact recreation.
Driving, desk work, and physical labor resume when your OSI provider confirms you are ready — based on motion, strength, and how the knee tolerates load, not on a fixed calendar. Venous thromboembolism prophylaxis is standard. Numbness along the incision is common early on and usually fades over time.
When to Contact Us
making the callCall (830) 625-0009
Schedule an evaluation for knee pain that has persisted beyond six weeks, limits walking or stairs, wakes you at night, or no longer responds to over-the-counter medication. Call sooner for a locked knee, sudden inability to bear weight, fever with joint pain, or a painful swollen joint after trauma.
Providers Who Treat Knee Osteoarthritis
joint-replacement team

David B. Templin, M.D.

Trent Twitero, M.D.
Further Reading
authoritative sourcesExternal patient-education references and related OSI pages for additional background: