Overview
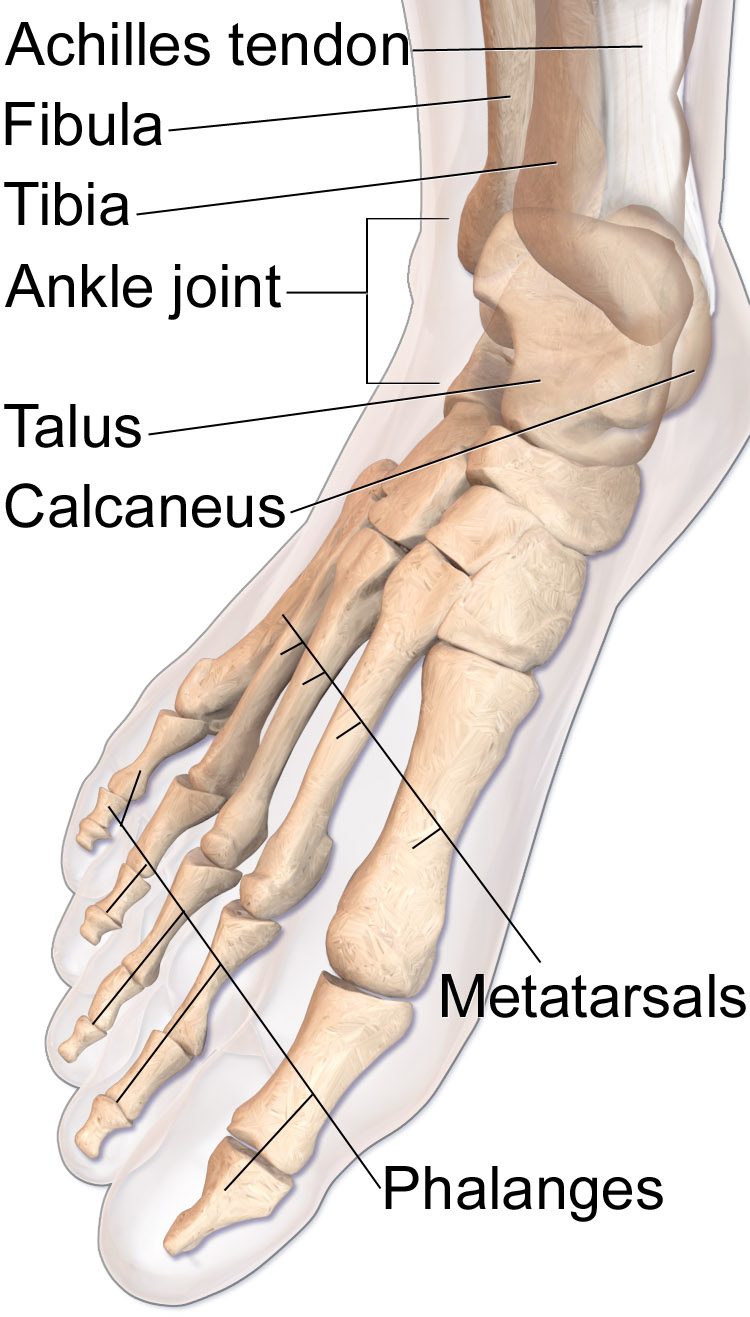
A pilon fracture is a break at the bottom of the tibia that crosses into the ankle joint. These are typically high-energy injuries with significant soft-tissue swelling, skin compromise, and joint comminution. Rushing to definitive fixation through swollen skin leads to very high wound-complication rates.
For these reasons, most pilon fractures are managed in two stages: first, a spanning external fixator is placed to restore length and alignment while the soft tissues rest; then, after one to three weeks, definitive plate-and-screw fixation is performed once the skin has calmed down.
Why it's done
Pilon fracture ORIF is typically considered when imaging and the clinical picture together indicate that the fracture will not reliably heal or function without surgical stabilization. Common indications include:
Displaced intra-articular fracture
Joint step-off accelerates ankle arthritis.
Angulation or shortening of the tibia
Alignment must be restored for normal walking mechanics.
Open fracture
Urgent debridement and external fixation.
Associated fibular fracture
Often fixed at the same time.
Skin compromise
Delayed-staged fixation minimizes wound complications.
How it works
Stage one is a spanning external fixator placed across the ankle — pins in the tibia above and the foot below, with bars connecting them. Length, alignment, and rotation are restored.
Stage two is definitive fixation once the soft tissues allow. Through carefully planned incisions, the distal tibia is exposed, the joint surface reconstructed with small screws, and a plate or plates applied to the medial and/or anterolateral tibia.
Recovery
Strict non-weight-bearing is typical for ten to twelve weeks. Early ankle motion begins once the wound is stable. Physical therapy focuses on restoring subtalar and ankle motion. Despite good reduction, pilon fractures carry one of the highest rates of post-traumatic arthritis of any extremity injury. Ankle fusion or replacement may become a consideration many years later if symptomatic arthritis develops.
Contact
For questions about this procedure or to schedule an evaluation, call the office at (830) 625-0009 or request an appointment online.
Further Reading
External patient-education references and related OSI pages for additional background: