Overview
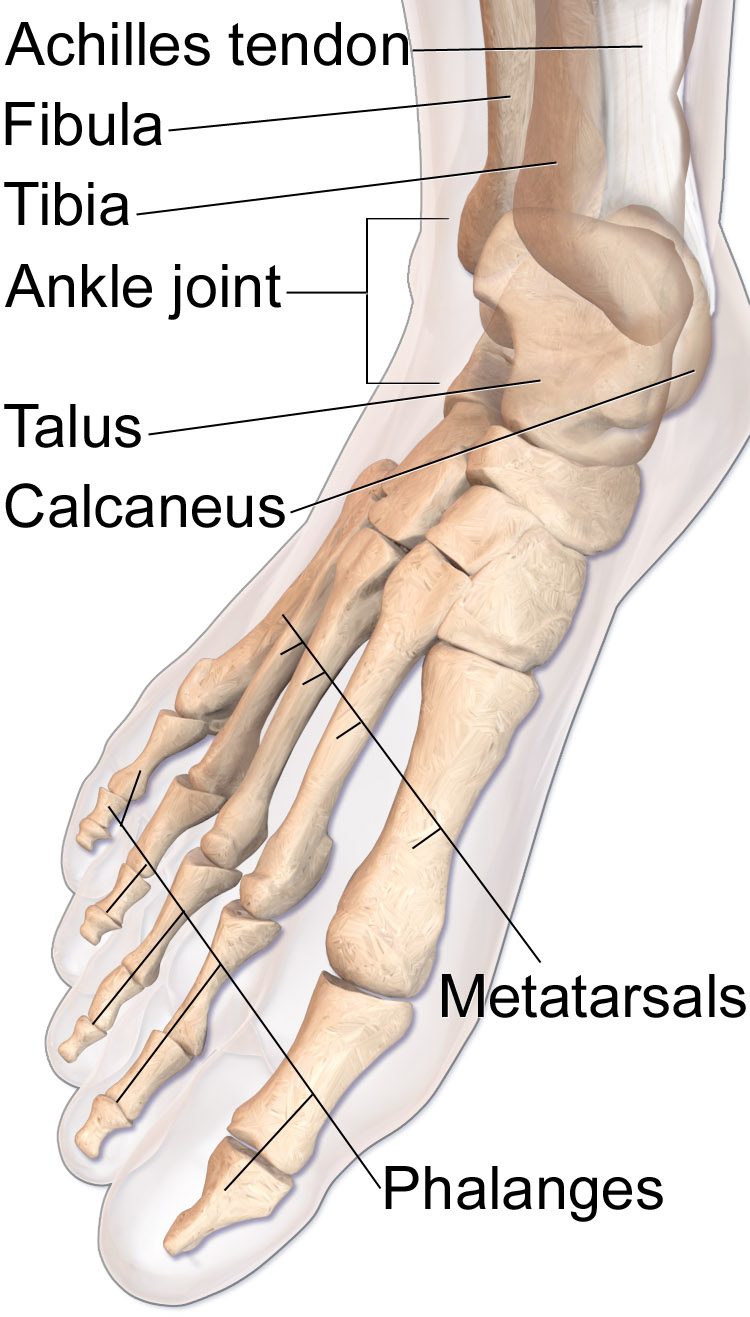
The calcaneus is the largest bone in the foot and carries the full load of body weight with every step. Most calcaneus fractures follow axial-loading injuries — typically falls from height — and often drive into the subtalar joint.
Operative fixation is considered for displaced intra-articular fractures, significant loss of heel height, or a widened heel that will not fit in a shoe. The goal is to restore the subtalar joint surface and the overall shape of the heel, since both are critical for normal hindfoot mechanics.
Why it's done
Calcaneus ORIF is typically considered when imaging and the clinical picture together indicate that the fracture will not reliably heal or function without surgical stabilization. Common indications include:
Displaced intra-articular fracture
Step-off in the subtalar joint surface drives early arthritis.
Loss of calcaneal height
A shortened heel changes ankle mechanics and shoe fit.
Widened or laterally displaced tuberosity
A wide heel impinges against the peroneal tendons and the fibula.
Tongue-type fractures threatening the skin
Displaced tongue fragments can tent the skin and need urgent reduction.
How it works
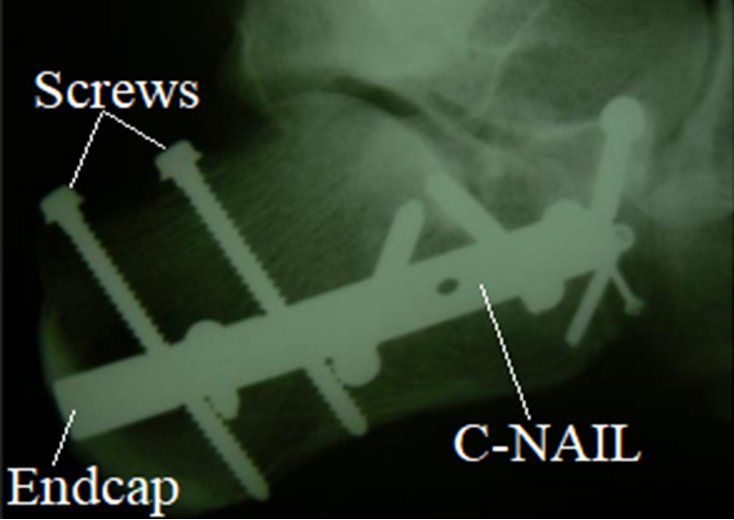
Traditional fixation uses an extensile lateral approach with a pre-contoured calcaneus plate and multiple screws once the soft tissue has rested and the swelling has come down. This gives the best visualization of the posterior facet.
Minimally invasive sinus-tarsi approaches with percutaneous screw fixation are used in selected patterns to reduce wound complications. Fluoroscopy and direct inspection confirm that the subtalar joint surface is smooth and the overall calcaneal shape is restored.
Recovery
Patients are splinted initially, then placed in a boot. Strict non-weight-bearing is standard for ten to twelve weeks because the calcaneus loads with every step. Range-of-motion exercises for the ankle and subtalar joint begin once the wound is healed. Graduated weight-bearing starts around three months. Despite a good reduction, post-traumatic subtalar arthritis remains a known long-term risk, and subtalar fusion may be considered later if symptoms develop. Hardware is removed only if it becomes symptomatic.
Contact
For questions about this procedure or to schedule an evaluation, call the office at (830) 625-0009 or request an appointment online.
Further Reading
External patient-education references and related OSI pages for additional background: