Overview
what it is and why it mattersPlantar fasciitis is pain at the bottom of the heel caused by irritation of the thick band of tissue that runs from the heel bone to the base of the toes. That band, called the plantar fascia, supports the arch of the foot. When it is overloaded — by new activity, extra body weight, long hours standing, tight calves, or simply time — small micro-injuries accumulate where the band attaches to the heel. The foot’s attempt to repair the damage, layered on top of continued use, becomes the nagging heel pain most people recognize as the “first step out of bed in the morning” ache.
About 1 in 10 adults will experience plantar fasciitis at some point in life. It is the most common reason adults see a foot-and-ankle specialist for heel pain. Most people get better with unhurried, consistent conservative care over several months. Surgery is rarely needed — fewer than 1 in 20 patients reach that point.
- 1 in 10adults, lifetime
- 6–12 mo.typical recovery
- >90%resolve without surgery
- 30–60typical age range
Anatomy: the band you stand on
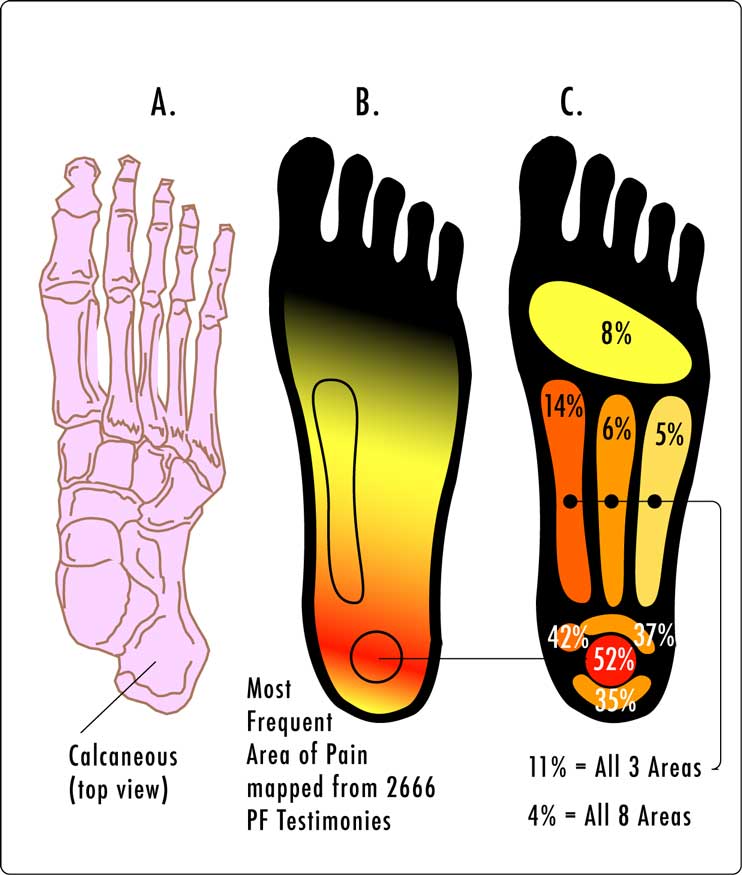
The plantar fascia is a sheet of collagen — the same kind of tough fibrous tissue that makes up tendons and ligaments. It runs from the underside of the heel bone (the calcaneus) to the base of each toe. When the toes are pushed up during walking, the band tightens and raises the arch, which is how a soft, flexible foot becomes a stiff lever that can push off the ground. Orthopedic surgeons call that stiffening action the windlass mechanism, after the hand-cranked winch it resembles.
In plantar fasciitis, the part of the band that takes the most load — right at the inside edge of the heel — gets micro-torn faster than the body can repair it. Over time the tissue becomes thickened and disorganized rather than inflamed, which is why many clinicians now call the fully chronic form plantar fasciosis. The pain and the treatment are the same.
What It Feels Like
the pattern of the painPlantar fasciitis has a recognizable rhythm most patients describe the same way, almost word for word:
- The first step out of bed is the worst. Sharp, stabbing, sometimes so bad patients limp for the first ten or twenty paces.
- It loosens up after a few minutes of walking — the fascia warms and stretches — then quietly backs off.
- It returns the longer you’re on your feet. Standing at a counter, a concert, a long shift, pushing a cart through a store — the dull ache creeps back in.
- Standing up after sitting is a mini-version of the morning. Any stretch of non-loading lets the fascia tighten; the first steps reload it painfully.
- Pain is on the inside and underside of the heel, usually one foot at a time, occasionally both.
- Barefoot on hard floors is worse. Tile, hardwood, concrete — anything that doesn’t give under the heel.
- No redness, warmth, or swelling. The top of the foot looks normal. The pain is inside the tissue, not on the skin.
What it isn’t
Plantar fasciitis hurts under the heel with first steps. Pain on the back of the heel is usually Achilles-related. Burning, tingling, or numbness that radiates into the toes points toward a nerve cause (tarsal tunnel syndrome). Pain after a single hard impact — missing a step, landing on a rock — is more likely a heel bone bruise or a stress fracture. If any of those fit better, the treatment is different; say so at the visit.
How It Starts
who tends to get it, and whyPlantar fasciitis is an overuse problem: the tissue is being loaded faster than it heals. Almost every case has at least one of these ingredients in the history — often several stacked together:
- New or increased activity
- Starting a walking habit, signing up for a 5K, a new job that keeps you on your feet — anything that changes the daily load on the heel. The fascia adapts, but slowly. Jumping the dose too fast is the single most common trigger.
- Extra body weight
- Body weight rides on the arch with every step. Even a modest gain changes the force across the fascia, and carrying it for years wears the tissue down. Weight loss is one of the most reliable long-term treatments.
- Tight calves
- A tight Achilles pulls the heel up and shifts load forward onto the arch. Daily calf stretching is the closest thing there is to a “single treatment that fixes it.”
- Age
- The fascia loses elasticity from the mid-thirties onward. Peak age is 40 to 60, though teenagers and eighty-year-olds can get it.
- Jobs on hard floors
- Teachers, nurses, retail, warehouse, restaurant, assembly line — anyone who logs thousands of steps on concrete, tile, or hardwood. Shoes with worn-out midsoles magnify the effect.
- Very flat or very high arches
- Both load the fascia differently from a neutral arch. Neither is destiny — plenty of flat-footed people never get it — but both raise the risk, especially when paired with the items above.
- Shoes past their life
- Running shoes and work shoes lose their cushion long before the uppers wear out. A shoe at 500 miles is not doing what it did at 50.
How We Make the Diagnosis
exam first, imaging only if neededPlantar fasciitis is a clinical diagnosis — meaning the history and physical exam are usually enough. A trained foot-and-ankle clinician can confirm it in a few minutes without any scan. A typical visit looks like this:
- The story. When did it start, what changed (new activity, new shoes, new weight, new job), when in the day is it worst, how long has it been going, what makes it better.
- Press the heel. Point tenderness right where the band meets the inside of the heel bone is the signature finding. Press elsewhere on the foot and the pain disappears.
- Toes-up test. Bend the big toe upward while the foot is relaxed. This tightens the fascia (the windlass mechanism) and usually reproduces the pain.
- Watch you walk. Gait, arch height, calf flexibility, and the wear pattern on your shoes all shape the plan.
Imaging is only ordered when something doesn’t fit. Most people with plantar fasciitis never need an X-ray or MRI.
Myth: “The X-ray shows a heel spur — that’s what’s causing the pain.”
Fact: Heel spurs and plantar fasciitis are separate findings that often travel together. Roughly a quarter of people with perfectly painless heels have spurs on X-ray. The spur is a marker of long-standing traction on the bone, not the source of the pain. Removing the spur does not cure plantar fasciitis; treating the fascia does.
When we do image:
- Ultrasound shows the fascia thickening (over 4 mm at the heel) and is used to guide injections precisely into the right layer.
- X-ray is used to rule out a heel stress fracture when the pain came on suddenly or doesn’t fit the usual pattern.
- MRI is reserved for atypical cases — pain that doesn’t respond to months of correct treatment, or a concern for a nerve entrapment or stress injury.
How We Treat It
what we try first, in orderThe single most important thing to know: plantar fasciitis is slow but reliable. With consistent conservative care, the large majority of patients are substantially better by six months and fully better by twelve. The treatments below are listed in the order we usually introduce them — each one is added on top of the ones before, not instead of.
Daily stretching
The single most effective conservative treatment. A plantar-fascia-specific stretch (foot crossed over the opposite knee, toes pulled back toward the shin, held 10 seconds, 10 reps) plus calf stretching, done before the first step of the day and two to three more times during the day. Consistency over months matters more than intensity in any one session.
Night splint
A soft brace worn while sleeping that holds the ankle at ninety degrees so the fascia can’t shorten overnight. Makes the first-step pain much milder within one to two weeks. Not everyone tolerates sleeping in one — that’s fine, it’s optional.
Heel cushion or supportive insole
A gel heel cup or a prefabricated arch-supporting insole in everyday shoes reduces the peak strain on the fascia with each step. Custom orthotics are an option but almost never the first one — off-the-shelf inserts work for most people and are a fraction of the cost.
-
Physical therapy
A structured program: eccentric loading of the calf and fascia, intrinsic foot-muscle strengthening, manual therapy, and gait coaching. Usually 4 to 8 sessions over 6 to 8 weeks. Most effective when started early and paired with the home stretching.
-
Anti-inflammatory pills, used briefly
Over-the-counter ibuprofen or naproxen can quiet a flare for one to two weeks but isn’t a long-term solution. The underlying tissue needs time and load, not continuous medication.
-
Cortisone injection
A targeted, ultrasound-guided injection into the right tissue layer can break a stubborn flare. We use it judiciously: repeated injections risk weakening the fascia, and one injection with correct technique is often enough. Relief typically lasts weeks to months and is meant to create a window for stretching and rehab to catch up.
-
Platelet-rich plasma (PRP)
An injection made from a small sample of your own blood, concentrated to deliver growth factors to the damaged tissue. Evidence is strongest in chronic cases that haven’t responded to three to six months of conservative care. More durable than cortisone for many patients; out-of-pocket cost in most practices.
-
Extracorporeal shock wave therapy (ESWT)
Focused sound-wave pulses applied to the heel, typically in 3 to 5 sessions, that stimulate healing in the fascia insertion. Reserved for chronic cases (past the three-month mark) not improving with stretching and PT. Not painful during treatment; mild soreness for a day after is common.
-
Weight, shoes, and surface
Three background levers that quietly determine whether the other treatments stick: modest weight loss when it applies, current-generation supportive shoes at home and at work, and limiting barefoot time on hard floors until the pain is fully resolved.
Recovery: What to Expect, Week by Week
a realistic timelineThe hardest part of plantar fasciitis is not the treatment — it’s the patience the tissue requires. The fascia heals on its own schedule, not the patient’s. Here is the realistic pace:
- Weeks 1–2
Start daily stretching and the night splint. Buy the heel cup. Shoes get reviewed. Pain is unchanged to slightly better; stick with it.
- Month 1
Morning pain starts softening. Standing tolerance lengthens. Physical therapy may be added.
- Months 2–3
Noticeably better. Most people return to most activities. Stretching stays daily — stopping now is the most common reason it comes back.
- Months 3–6
If still stuck, an ultrasound-guided cortisone injection, ESWT, or PRP is considered. Most patients are comfortable again by the 6-month mark.
- Months 6–12
For the minority who haven’t fully recovered, we keep escalating non-operative care. Full resolution at 12 months is typical even in stubborn cases.
- 12+ months
Surgical consultation is reasonable if pain remains disabling and imaging confirms the diagnosis. This is a small minority of cases.
When Surgery Is on the Table
uncommon — and a last stepSurgery for plantar fasciitis is reserved for patients who, after at least twelve months of correctly applied non-operative care, remain significantly limited by the pain. That threshold is not arbitrary: the fascia’s natural healing arc is about a year, and most patients who feel “stuck” at three or six months are better by twelve without any procedure. Jumping to surgery early has higher complication rates and does not improve long-term outcomes.
Keeping It From Coming Back
after you’re betterPlantar fasciitis recurs in roughly one in five people, usually because the conditions that caused it the first time didn’t change. Once the pain is gone, these habits have the biggest effect on keeping it gone:
- Don’t stop stretching. Calves and fascia, a few times a week, indefinitely. The tissue loses flexibility over weeks.
- Ramp activity gradually. When starting or returning to walking, running, hiking, or a new job on your feet, keep the weekly increase under about 10–15 percent.
- Replace shoes on miles, not looks. Running shoes around 400 to 500 miles. Daily work shoes roughly once a year.
- Respect hard floors. At home, keep a cushioned mat in spots where you stand a lot (kitchen, bathroom). Avoid long barefoot stretches on tile and hardwood.
- Manage weight steadily. Even a few pounds changes the force across the fascia.
Frequently Asked
questions we hear in clinicHow long until I’m better?
Most people are substantially better by three to six months of consistent stretching and basic conservative care, and fully better by twelve months. “Better” doesn’t mean perfect on day 30 — it means the morning pain softens, standing tolerance grows, and the weeks start to add up in your favor.
Do I need an MRI?
Almost never. Plantar fasciitis is diagnosed from the history and the exam. An MRI is reserved for cases that don’t respond to months of correct treatment or where something in the exam doesn’t fit.
Can I keep running?
Often yes, if the pain stays mild and doesn’t get worse the day after. Cut weekly mileage, switch some runs to a softer surface, and make sure the shoes are fresh. If the pain is sharp or limping-level, take a break and rebuild.
When should I get a cortisone injection?
When you’ve been diligent with stretching, the night splint, and shoe changes for at least a couple of months and the pain is still interfering with daily life. An injection done right creates a window for the other treatments to catch up. Jumping to an injection week one is not the right order.
Are custom orthotics worth it?
For most people, no — not as a first step. A good over-the-counter heel cup or arch support is usually enough. Custom orthotics become reasonable when off-the-shelf hasn’t helped after a few months, or when foot shape is very unusual.
I heard I have a heel spur. Do I need that removed?
No. The spur isn’t the pain generator; the fascia is. Plenty of people have spurs on X-ray and no heel pain at all. Treat the fascia; leave the spur alone.
Can kids get plantar fasciitis?
Very rarely. Heel pain in children is usually Sever’s disease, which is a growth-plate issue and is treated differently.
Further Reading
authoritative sourcesExternal patient-education references and related OSI pages for additional background: