Overview
what it is and why it matters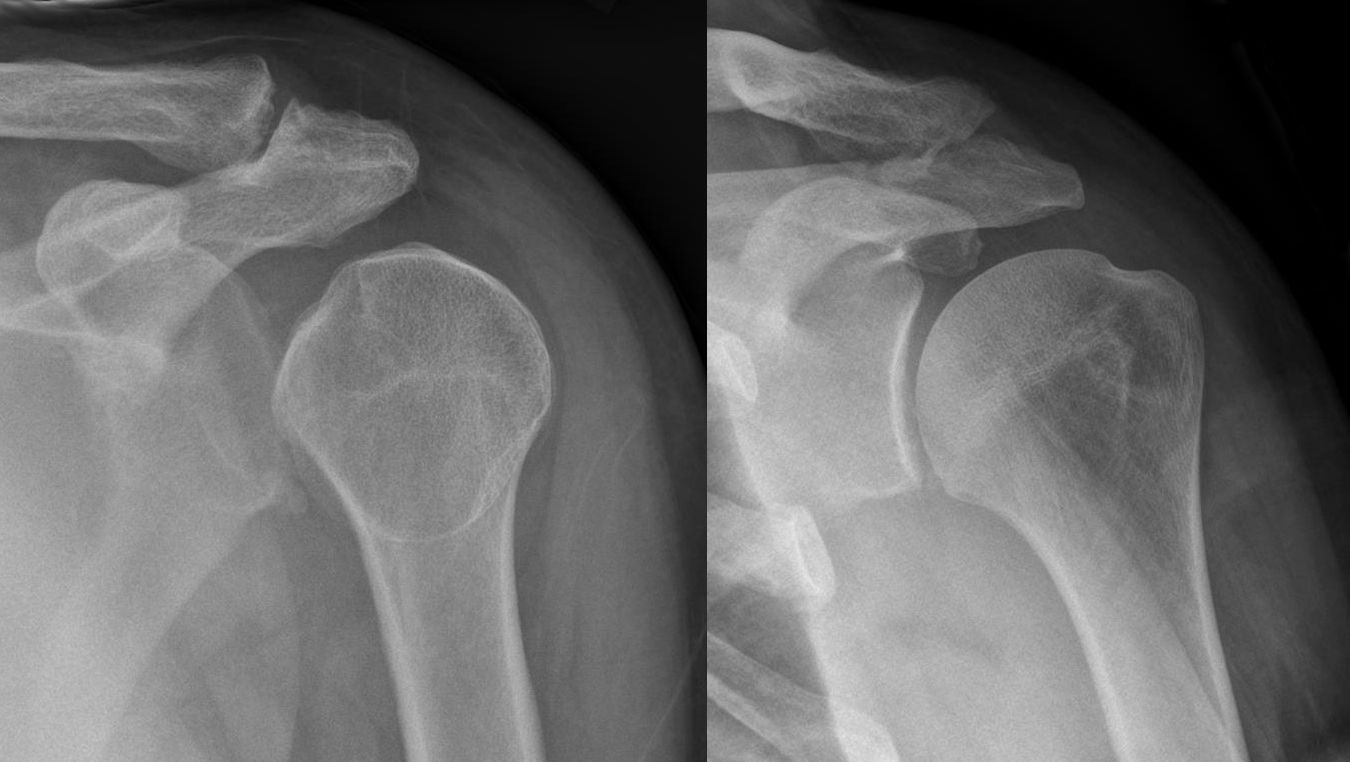
Posterior shoulder instability — where the humeral head displaces posteriorly — accounts for approximately 5–10% of all shoulder instability. It is most common in weight lifters (bench press), football linemen, and swimmers, and is frequently missed because the presentation is less dramatic than anterior instability. Voluntary posterior subluxation (intentional self-positioning of the shoulder to cause it to slip) is a distinct entity often associated with psychological factors.
Diagnosis
exam first, imaging secondPain and a "dead arm" sensation with the arm in forward flexion, adduction, and internal rotation — the "at-risk" position for posterior instability. The posterior load-and-shift test and the jerk test confirm posterior laxity. MRI arthrography evaluates the posterior capsule, posterior labrum (reverse Bankart), and glenoid retroversion.
Treatment Path
how care progresses at OSI1
Physical therapy
Posterior rotator cuff and periscapular strengthening — the primary treatment for posterior instability and highly effective in many cases.
2
Activity modification
Avoiding provocative positions (deep bench press, heavy overhead push) during rehabilitation.
Surgical Options at OSI
if non-operative care isn't enoughCases unresponsive to 6 months of dedicated rehabilitation in which structural posterior labral tears are confirmed on imaging are considered for surgical repair.
Providers Who Treat Posterior Shoulder Instability
sports-medicine team

David B. Templin, M.D.

Trent Twitero, M.D.
Further Reading
authoritative sourcesExternal patient-education references and related OSI pages for additional background: