Overview
what it is and why it matters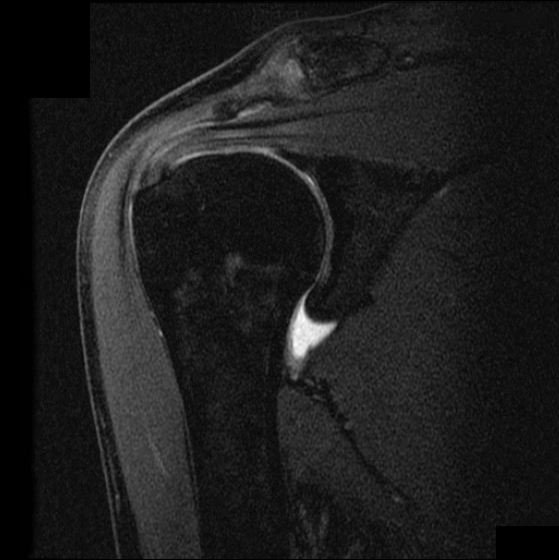
The rotator cuff is a group of four tendons — supraspinatus, infraspinatus, teres minor, and subscapularis — that wrap around the humeral head (the ball of the shoulder) and hold it centered in the glenoid (the socket). They are the muscles that let you raise, rotate, and control the arm with precision. When one tears, the arm loses its coordinated pull and the shoulder can no longer position itself reliably against gravity. Most tears involve the supraspinatus, the tendon that runs across the top of the joint, and range from partial fraying to complete detachment from the bone.
Tears divide into two patterns. Acute tears follow a single event — a fall onto the arm, a heavy lift, or a shoulder dislocation in a younger patient. Degenerative tears accumulate over years as the tendon thins and frays under repeated use, typically in middle-aged and older adults. After age 60, a torn rotator cuff seen on imaging often represents normal wear rather than a true injury, which is why the symptoms and the findings must be interpreted together.
Anatomy & Mechanism
why these tendons tearThe supraspinatus passes beneath the coracoacromial arch as it inserts on the greater tuberosity. The subacromial space — bounded by the acromion above and the humeral head below — narrows with arm elevation, and the tendon is exposed to compressive and shear loads. Chronic impingement and intrinsic tendon degeneration together weaken the tendon over decades. A relatively minor force can then complete a tear in an already-degenerated tendon.
Size matters for treatment: small tears often behave differently from large or retracted tears with muscle atrophy and fatty infiltration (Goutallier and Fuchs grading on MRI). These features, together with the patient's age, activity demands, and hand dominance, drive the decision to repair.
Symptoms
what patients describe- Lateral shoulder and upper arm pain, often worse at night and with overhead activity
- Weakness lifting the arm away from the body or reaching overhead
- Difficulty sleeping on the affected side
- Pain with reaching behind the back (tucking a shirt, fastening a bra, reaching a seatbelt)
- Crepitus or popping with shoulder motion in some patients
Diagnosis
exam first, MRI secondExamination localizes the torn tendon: the empty-can (Jobe) test assesses the supraspinatus, external-rotation lag and hornblower's signs target the infraspinatus and teres minor, and the lift-off and belly-press tests assess the subscapularis. Weakness out of proportion to pain suggests a structural tear rather than inflammation alone.
Plain X-rays are obtained to evaluate for proximal humeral migration (a marker of a chronic, massive tear), subacromial spurring, and calcific tendinopathy. MRI is the imaging standard: it defines tear thickness, tear dimensions, tendon retraction, and the degree of muscle atrophy and fatty infiltration — all of which predict reparability and outcome.
Nonoperative Treatment
effective for most patientsStructured physical therapy is first-line for most patients with rotator cuff tears, including many with full-thickness tears. The majority who commit to a genuine course of therapy avoid surgery and regain durable comfort even when imaging still shows the tear.
1
Physical therapy
Strengthening the intact cuff tendons, the deltoid, and the muscles that anchor the shoulder blade restores balanced shoulder mechanics and often provides lasting relief even with a structural tear present.
2
Anti-inflammatory medication
A short course of ibuprofen, naproxen, or a similar anti-inflammatory addresses the inflammatory component and allows fuller participation in therapy.
3
Cortisone injection
A single cortisone injection into the subacromial space above the cuff can provide weeks to months of pain relief and is useful when pain prevents progress in therapy. Repeated injections near an intact tendon are avoided, because steroid can weaken tendon tissue over time.
Operative Treatment
who benefits from repairSurgery is considered for acute full-thickness tears in active patients, for tears with significant weakness limiting function, for tears that have not improved with a structured nonoperative trial, and for large tears at risk of propagation or muscle atrophy that would compromise future repair. In selected patients with chronic irreparable cuff tears and cuff-tear arthropathy, reverse shoulder replacement restores overhead function by recruiting the deltoid.
Primary procedure
Rotator cuff repair
Arthroscopic reattachment of the torn tendon to its footprint using suture anchors. Protected sling use is required during tendon-to-bone healing.
Learn about this procedure →Additional option
Reverse shoulder replacement
Reverses the ball-and-socket so the deltoid can substitute for a deficient rotator cuff. Reserved for chronic irreparable tears, cuff-tear arthropathy, and selected revisions.
Learn about this procedure →Recovery & Expectations
protecting the repairAfter rotator-cuff repair, recovery is deliberately slow — tendon healing to bone takes time, and rushing it puts the repair at risk. The early phase uses a sling with gentle, passive motion only; active use of the arm is held back until healing is established. Active-assisted and then active motion come next, followed by progressive strengthening. Return to overhead work, heavy lifting, and sport is the final phase and depends on how the repair has healed.
Structural healing rates depend on tear size, tissue quality, and patient age. Many patients feel well even when imaging shows incomplete healing — symptomatic outcomes often exceed structural outcomes. Your OSI provider advances you through each phase based on exam and comfort, not on a fixed calendar.
When to Contact Us
making the callCall (830) 625-0009
Schedule an evaluation for shoulder pain that limits reaching overhead or away from the body, wakes you at night, or has not improved after two to four weeks of rest and over-the-counter anti-inflammatories. Call sooner for weakness after a fall or lifting injury, or for pain accompanied by deformity, numbness, or a cold, pale hand.
Providers Who Treat Rotator Cuff Tear
sports-medicine team

David B. Templin, M.D.

Trent Twitero, M.D.
Further Reading
authoritative sourcesExternal patient-education references and related OSI pages for additional background: