Overview
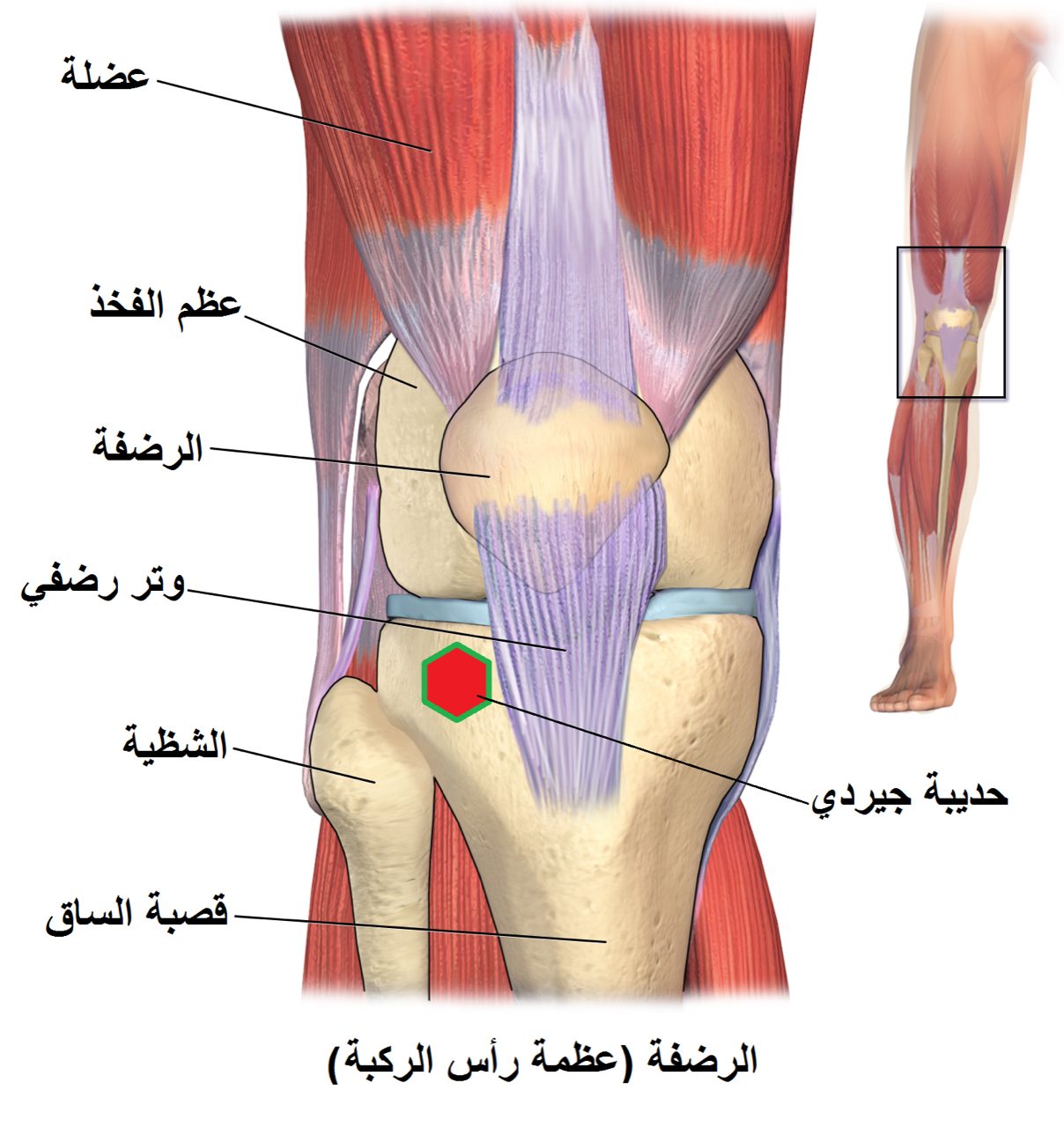
The knee is a hinge joint where the femur, tibia, and patella articulate through three compartments of cartilage. When that cartilage wears through across multiple compartments — the hallmark of tricompartmental osteoarthritis — standing, walking, and stairs become painful and the leg can bow or buckle. Total knee replacement resurfaces the damaged ends of the bones.
How the Procedure Works

We remove the damaged cartilage and a measured layer of bone from the femur, tibia, and typically the back of the patella — no more than necessary, because bone removal is permanent. Metal components are cemented or press-fit onto the femur and tibia, with a polyethylene spacer between them. The part of the procedure that most affects the outcome isn't implant selection; it's gap balancing and alignment. We check flexion and extension gaps with trial components in place: if the knee is tighter in flexion than extension, or vice versa, we adjust the tibial cut and soft-tissue releases until both gaps match. A knee that is well-balanced and properly aligned will track smoothly, bear load evenly, and feel stable through the full arc of motion. One that is not will hurt and wear asymmetrically regardless of implant brand.
When to Consider Total Knee Replacement
Total knee replacement is generally offered when symptoms, imaging, and a trial of non-operative care together point to surgery as the next step. The typical picture includes:
Advanced tricompartmental arthritis
Cartilage loss across multiple compartments on weight-bearing X-rays, with daily pain and functional loss.
Exhausted non-operative care
Failed extended course of anti-inflammatories, physical therapy, weight loss, bracing, and intra-articular injections.
Deformity or instability
Progressive varus or valgus deformity, or a knee that buckles — both signal that the joint is no longer supporting the limb.
Conditions This Treats
Physicians Who Perform Total Knee Replacement


David B. Templin, M.D.

Trent Twitero, M.D.
Providers Who Surgically Assist with Total Knee Replacement

Sydney Georg, PA-C
Ben Swanner, PA-C
Further Reading
External patient-education references and related OSI pages for additional background: