Overview

Intertrochanteric fractures occur in the area of the hip between the greater and lesser trochanters, outside the hip capsule. Unlike femoral neck fractures, the blood supply to the femoral head is usually preserved, so the bone tends to heal when stabilized.
Surgery is almost always indicated. Rapid fixation allows the patient to get out of bed quickly, which is critical for elderly patients in whom prolonged bed rest carries a high medical-complication rate. Non-operative treatment is reserved for patients too frail to survive surgery.
Why it's done
Intertrochanteric fracture fixation is typically considered when imaging and the clinical picture together indicate that the fracture will not reliably heal or function without surgical stabilization. Common indications include:
Fracture displacement
Essentially all displaced intertrochanteric fractures are surgical.
Need for rapid mobilization
Early weight-bearing prevents pneumonia, blood clots, and pressure injuries.
Reverse-oblique or subtrochanteric extension
A cephalomedullary nail is usually required for these patterns.
Previous sliding hip screw cutout
Revision typically involves conversion to arthroplasty.
How it works
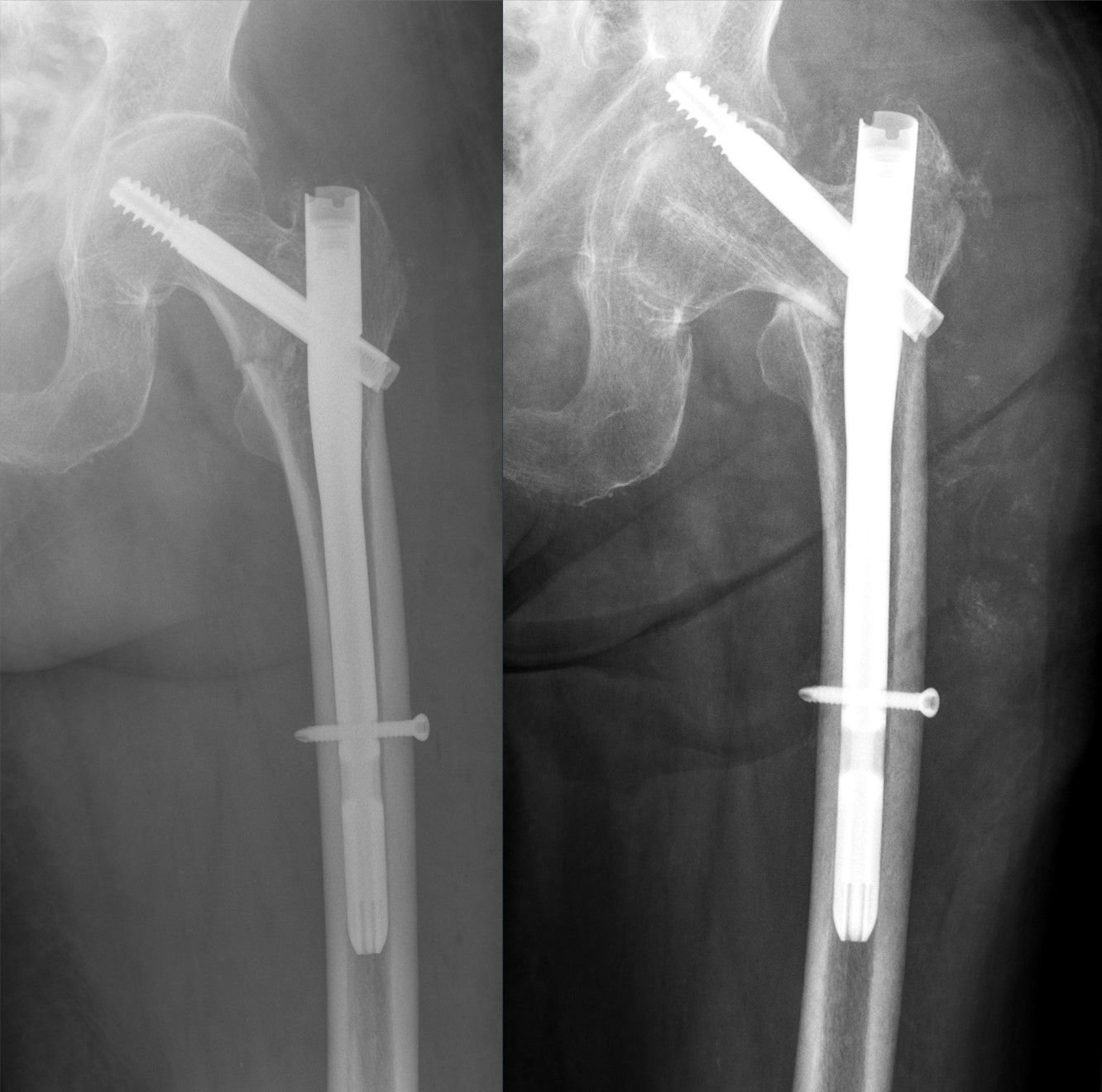
A cephalomedullary nail is placed through a small incision at the top of the hip. The nail is inserted down the femur and a large lag screw or helical blade is driven up into the femoral head. This implant resists the shear and bending forces across the fracture.
A sliding hip screw-and-plate construct is an alternative for simple stable patterns. Fluoroscopy is used throughout to confirm implant position.
Recovery
Most patients are allowed to weight-bear as tolerated on the first day after surgery and mobilized with a walker. Physical therapy in the hospital and at home focuses on regaining walking endurance. Union is typically seen by three months. Late complications to watch for include lag-screw cutout and nonunion, especially in highly comminuted patterns. Hardware is removed only if symptomatic.
Contact
For questions about this procedure or to schedule an evaluation, call the office at (830) 625-0009 or request an appointment online.
Further Reading
External patient-education references and related OSI pages for additional background: