Overview

The subtrochanteric region is the upper shaft of the femur just below the lesser trochanter. This area carries enormous bending and torsional loads with walking, which makes it one of the highest-stress sites in the skeleton. Fractures here are notorious for delayed union and implant failure if fixation is suboptimal.
These fractures also have a well-known association with long-term bisphosphonate use — so-called atypical femoral fractures — which present with a specific radiographic pattern and often require bilateral evaluation.
Why it's done
Subtrochanteric fracture fixation is typically considered when imaging and the clinical picture together indicate that the fracture will not reliably heal or function without surgical stabilization. Common indications include:
Virtually all displaced subtrochanteric fractures
Non-operative treatment cannot hold alignment.
Atypical femoral fracture
Prophylactic or therapeutic nailing is standard.
Pathologic fracture
Nailing provides pain control and stabilization.
Reverse-oblique pattern extending from above
Cephalomedullary nailing is strongly preferred.
Significant shortening or angulation
Restoration of length and alignment is essential.
How it works
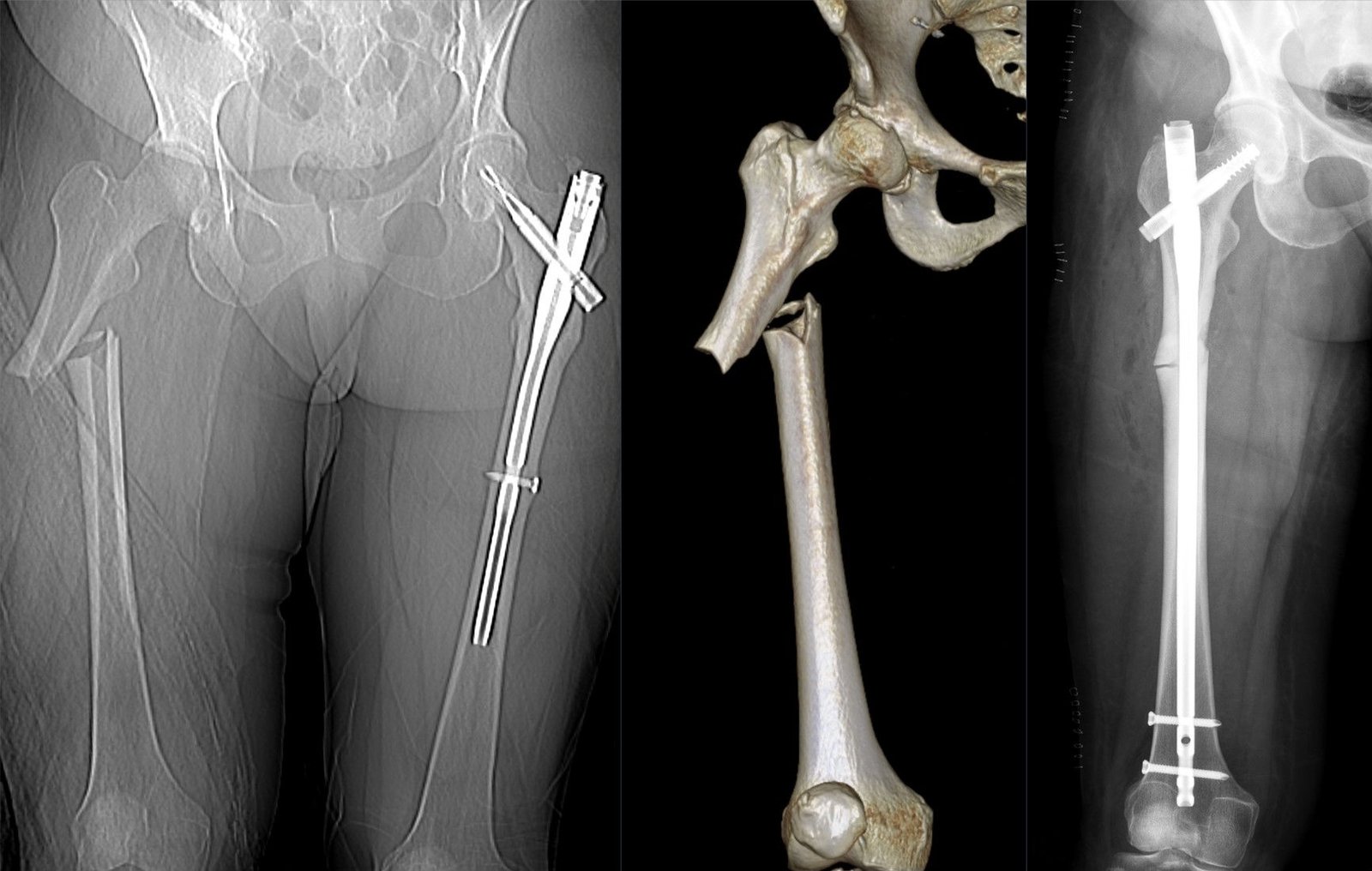
A long cephalomedullary nail is passed down the femur through a small incision at the top of the hip. A large lag screw or helical blade is driven up into the femoral head, and distal locking screws capture the shaft.
Reduction is critical in this region — particularly restoration of the medial cortical buttress, valgus alignment, and rotation — to minimize implant stress. Cerclage cables or wires are sometimes added for comminuted or oblique patterns.
Recovery
Protected weight-bearing is common for six to twelve weeks, especially in atypical femoral fractures, which are prone to delayed union. Hip and knee range-of-motion exercises begin early. Union takes three to six months on average, sometimes longer. Implant failure and nonunion remain risks if reduction is inadequate. Hardware removal is uncommon unless a specific problem develops.
Contact
For questions about this procedure or to schedule an evaluation, call the office at (830) 625-0009 or request an appointment online.
Further Reading
External patient-education references and related OSI pages for additional background: