Overview
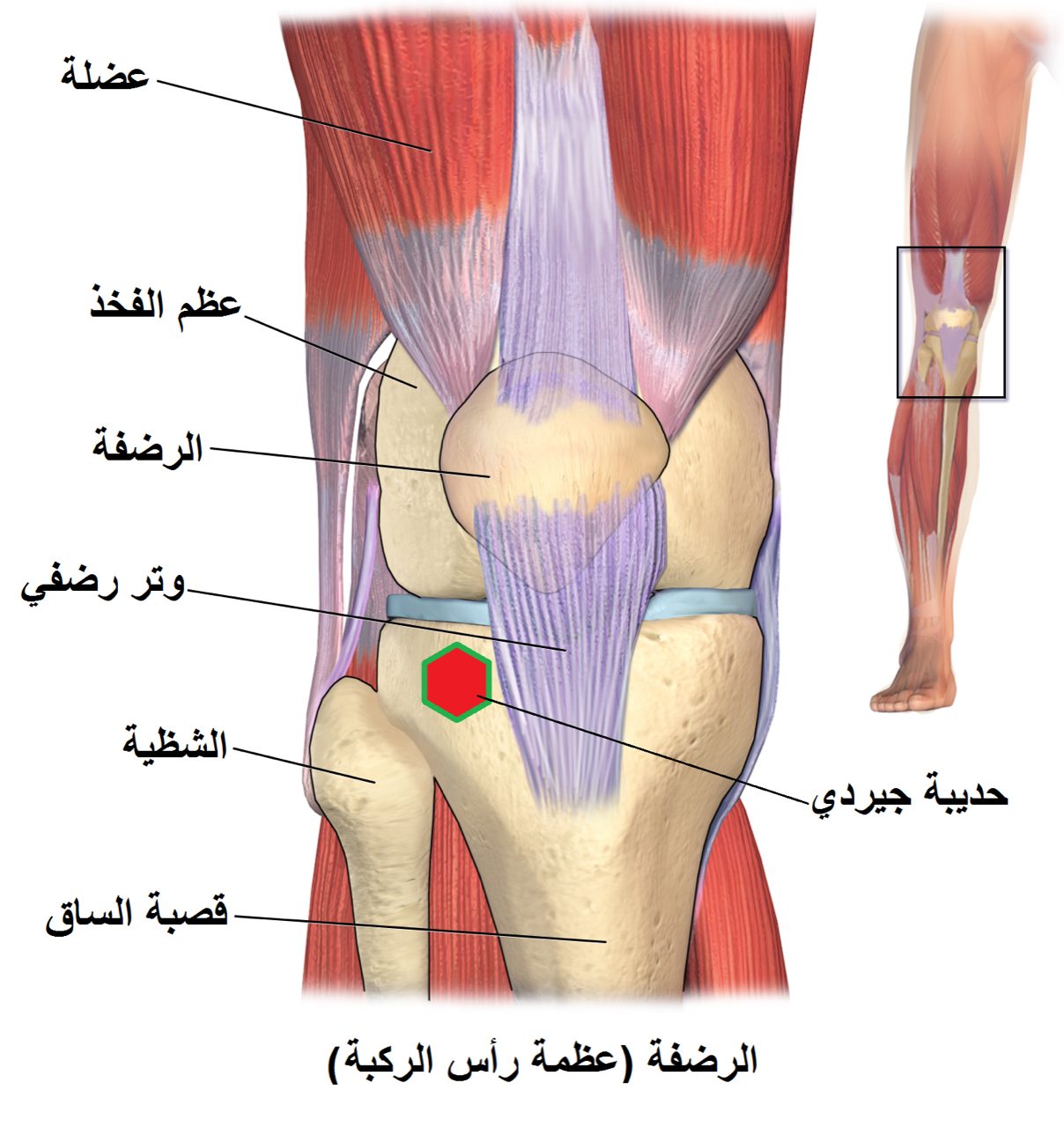
The medial and lateral menisci are C-shaped shock absorbers between the femur and tibia. Only the outer third has a reliable blood supply, so only certain tear patterns heal predictably. When the tear is in that vascular zone, suturing the meniscus back together — rather than trimming it away — protects the knee from the long-term arthritis that follows meniscectomy.
How the Procedure Works
We choose the suture technique based on tear location. All-inside devices work efficiently for posterior horn tears where percutaneous needles would risk the popliteal neurovascular structures; inside-out sutures, tied over a posteromedial or posterolateral capsular incision, give the strongest fixation and are preferred for mid-body tears; outside-in technique suits anterior horn tears. The torn edges are freshened with a rasp or trephine to stimulate a healing response before sutures are placed — a tear sutured without edge preparation heals less reliably. We place enough sutures to close the tear without gaps, then stress the repair through a range of motion before leaving the OR: if it opens under load, we add sutures. Concurrent ACL reconstruction actually helps meniscus repairs heal, likely through the marrow elements released during tunnel drilling, so we don't shy away from repairing a meniscus that might otherwise be trimmed when ACL reconstruction is also being done.
When to Consider Meniscus Repair
Meniscus repair is generally offered when symptoms, imaging, and a trial of non-operative care together point to surgery as the next step. The typical picture includes:
Traumatic longitudinal tear
A vertical tear in the peripheral, vascular zone of the meniscus — the pattern most likely to heal.
Younger patient, active lifestyle
Healing potential is higher and the long-term benefit of preserving the meniscus is greatest in patients with decades of activity ahead.
Root tears
Root avulsions functionally uncap the joint and should almost always be repaired rather than debrided.
Conditions This Treats
Physicians Who Perform Meniscus Repair


David B. Templin, M.D.

Trent Twitero, M.D.
Providers Who Surgically Assist with Meniscus Repair

Sydney Georg, PA-C
Ben Swanner, PA-C
Further Reading
External patient-education references and related OSI pages for additional background: