Overview
When the kneecap tracks too far laterally — or sits too high — the forces across the patellofemoral joint become abnormal and instability or wear follows. The attachment of the patellar tendon, the tibial tubercle, can be surgically moved to normalize those forces. The procedure is often combined with MPFL reconstruction when multiple anatomic factors contribute.
How the Procedure Works
We plan the direction and magnitude of the shift preoperatively using CT measurements — specifically the tibial-tubercle to trochlear-groove (TT-TG) distance for medialization, and the Caton-Deschamps ratio for distalization. The tubercle is cut as a long, tapered wedge of bone rather than a short block; the longer the osteotomy, the larger the contact surface for healing and the lower the stress per unit area at the fixation screws. We shift it the planned amount, confirm patellar tracking arthroscopically before fixing, and adjust if the patella still rides laterally or tilts. Two cortical screws hold the new position. When anteriorization is added — rotating the tubercle forward to offload a damaged patellar cartilage area — we plan that vector precisely so we don't inadvertently increase the Q-angle while trying to unload the joint surface.
When to Consider Tibial Tubercle Osteotomy
Tibial tubercle osteotomy is generally offered when symptoms, imaging, and a trial of non-operative care together point to surgery as the next step. The typical picture includes:
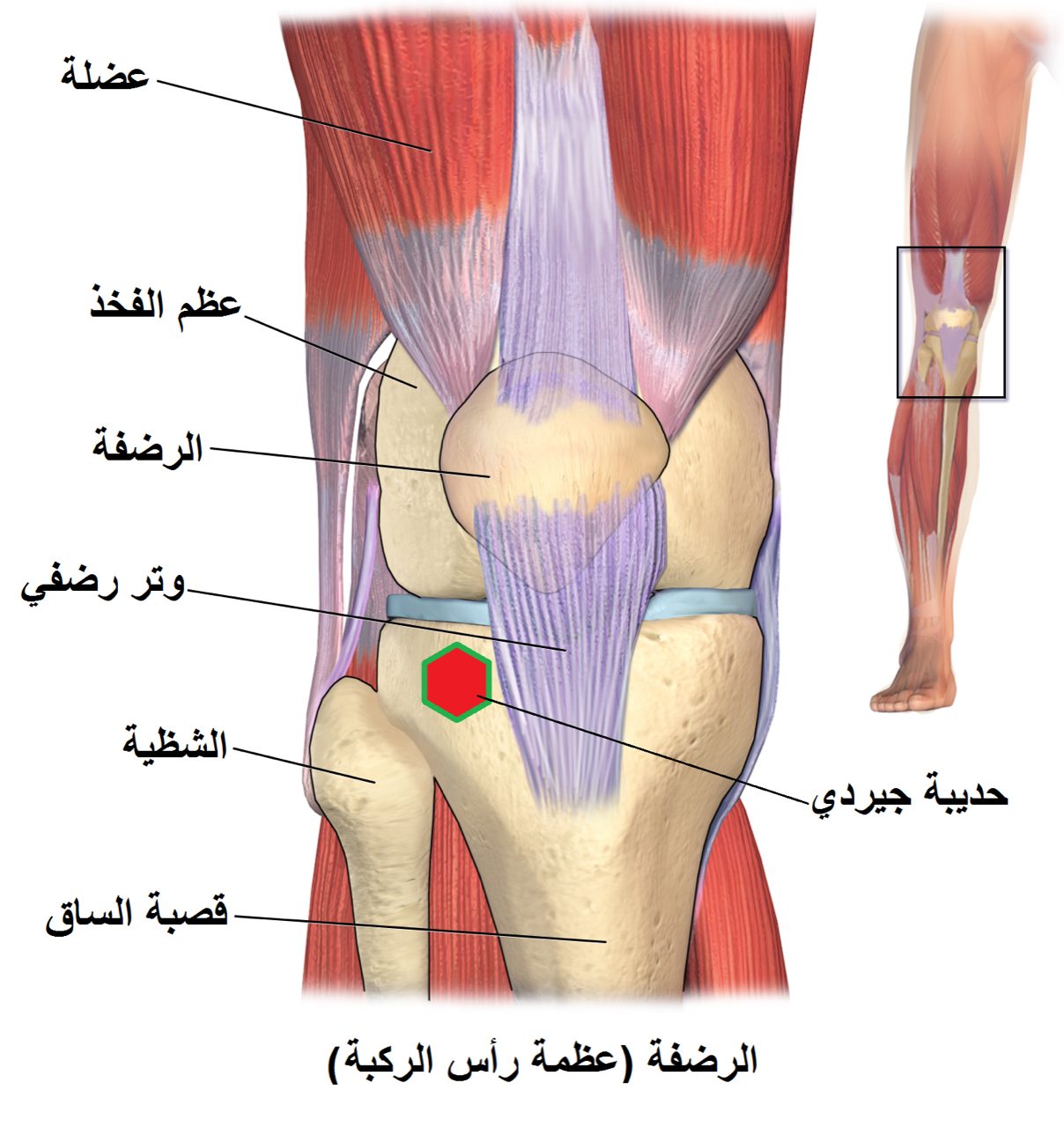
Instability with tubercle-trochlear offset
Imaging showing a lateralized tubercle that contributes to recurrent patellar dislocation.
Patella alta contributing to instability
A high-riding kneecap that engages the trochlea too late in flexion.
Patellofemoral arthritis realignment
Anteriorization or anteromedialization to unload a damaged area of patellar cartilage.
Conditions This Treats
Physicians Who Perform Tibial Tubercle Osteotomy


David B. Templin, M.D.

Trent Twitero, M.D.
Providers Who Surgically Assist with Tibial Tubercle Osteotomy

Sydney Georg, PA-C
Ben Swanner, PA-C
Further Reading
External patient-education references and related OSI pages for additional background: