Overview
what it is and why it matters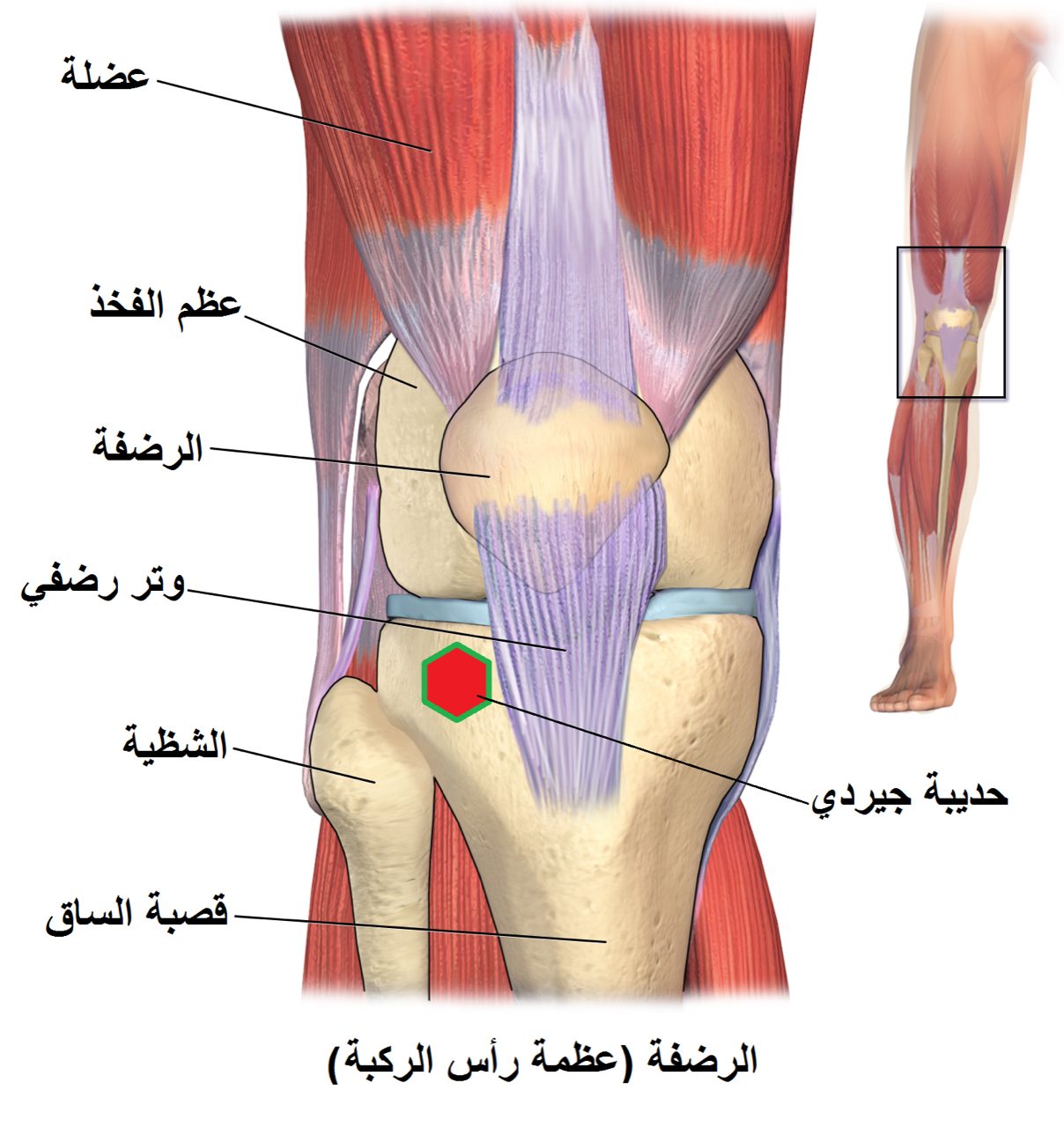
Patellar tendinopathy ("jumper's knee") is a painful overuse condition affecting the patellar tendon — the tendon connecting the kneecap (patella) to the tibial tubercle. Repetitive loading during jumping, landing, and accelerating causes micro-damage in the tendon that accumulates faster than it can repair, leading to a disorganized, degenerated tendon that is painful and less tolerant of load.
It is most common in basketball players, volleyball players, and high jumpers. The condition can become chronic and career-limiting if not managed appropriately early.
Diagnosis
exam first, imaging secondAnterior knee pain localized to the inferior pole of the patella — the patellar tendon origin — reproduced by pressing on that point. Pain typically occurs at the start of activity, may improve with warm-up, then return after exercise. MRI and ultrasound identify intratendinous degeneration, thickening, and neovascularization.
Treatment Path
how care progresses at OSI1
Load management
Reducing the volume and intensity of jumping activities — not complete rest, but carefully managed progressive loading.
2
Eccentric & heavy slow resistance training
Eccentric squats (decline squats) and heavy slow resistance training are the most evidence-based treatments. Stimulate tendon remodeling.
3
Patellar tendon strap / offloading brace
A strap just below the kneecap reduces load on the tendon origin and provides pain relief during activity.
PRP injection
Platelet-rich plasma injected into the tendon has evidence supporting its use in patellar tendinopathy, particularly when rehabilitation alone has not resolved symptoms.
Extracorporeal shock wave therapy (ESWT)
Non-invasive acoustic wave treatment with good evidence for chronic patellar tendinopathy.
Surgical Options at OSI
if non-operative care isn't enoughSurgery is a last resort, considered after at least 6–12 months of consistent loading program, PRP, and ESWT have failed.
Providers Who Treat Patellar Tendinopathy
sports-medicine team

David B. Templin, M.D.

Trent Twitero, M.D.
Further Reading
authoritative sourcesExternal patient-education references and related OSI pages for additional background: