Overview
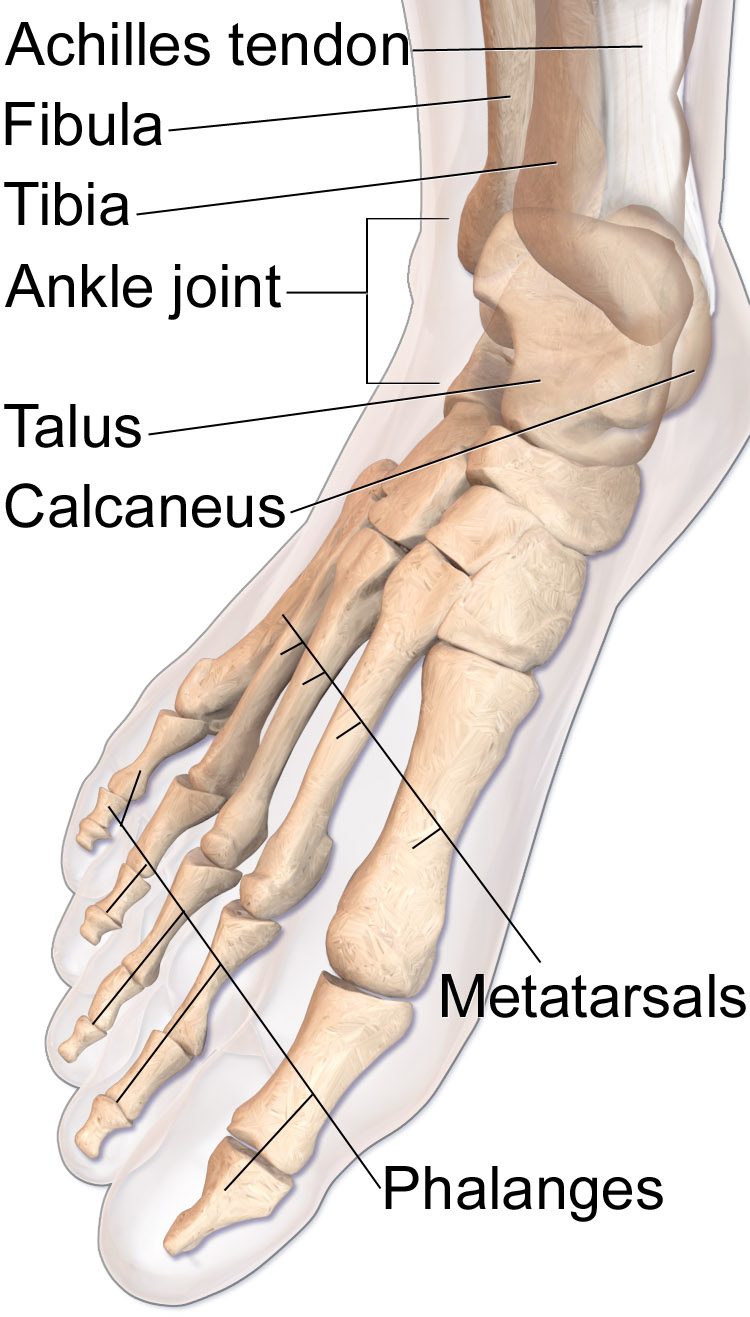
The ankle is a tight three-sided mortise formed by the fibula, tibia, and talus. When one or more of these bones break and the joint shifts out of alignment, the cartilage surfaces no longer match and uneven loading leads rapidly to arthritis.
Surgical fixation restores the mortise. Fractures that shift even a few millimeters, patterns that cross the joint, and injuries with syndesmotic (high-ankle) instability usually need surgery rather than a cast.
Why it's done
Ankle fracture ORIF is typically considered when imaging and the clinical picture together indicate that the fracture will not reliably heal or function without surgical stabilization. Common indications include:
Displaced fibular fracture
A fibula that sits short or rotated changes how the talus contacts the tibia.
Bimalleolar or trimalleolar pattern
Fractures involving both sides of the ankle are inherently unstable.
Syndesmotic disruption
Widening between the tibia and fibula requires fixation to restore the mortise.
Open fracture or skin compromise
Skin tension over the fracture may demand urgent reduction and fixation.
Talar shift on weight-bearing films
Any displacement of the talus under load is an indication to operate.
How it works
Lateral malleolar (fibula) fractures are reduced through an incision along the outer ankle and held with a contoured plate and screws. Medial malleolar fractures are fixed through a small incision on the inside of the ankle with screws or a small plate.
If the syndesmosis is unstable, one or two screws or a flexible suture-button implant is placed across the tibia and fibula to hold the bones together while the ligaments heal. Fluoroscopy is used throughout to confirm anatomic reduction.
Recovery
Patients are typically splinted for the first one to two weeks and transitioned to a boot. Weight-bearing is usually protected for six weeks after isolated fractures and longer if the syndesmosis was fixed. Physical therapy begins once the fracture is stable, focused on restoring motion and strength. Most patients return to walking without a boot by two to three months. Hardware is not routinely removed unless it becomes symptomatic.
Contact
For questions about this procedure or to schedule an evaluation, call the office at (830) 625-0009 or request an appointment online.
Further Reading
External patient-education references and related OSI pages for additional background: