Overview
what it is and why it matters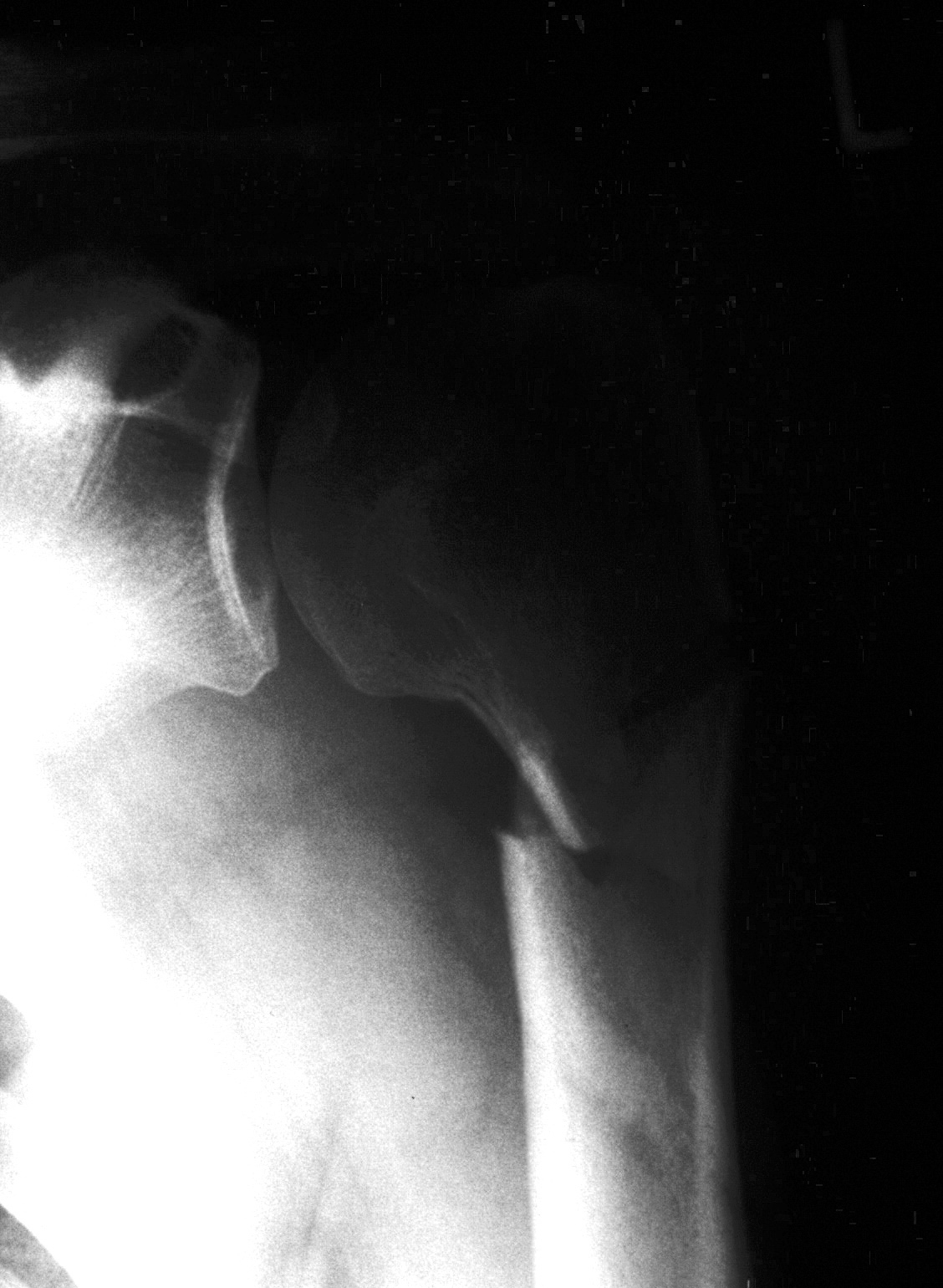
Proximal humerus fractures are among the most common fractures in adults over 65 — the third most common fracture type in the elderly after hip and distal radius fractures. They typically occur from a fall onto an outstretched arm or directly onto the shoulder. The Neer classification describes fractures based on the number of displaced segments (1–4 parts): the humeral head, greater tuberosity, lesser tuberosity, and shaft.
The vast majority — over 80% — are minimally displaced and heal well with non-operative management. Displaced multi-part fractures, particularly in younger patients, are a complex reconstructive challenge.
Diagnosis
exam first, imaging secondShoulder pain, swelling, and ecchymosis tracking down the arm and chest wall after a fall. Neurovascular assessment is critical — the axillary nerve is at risk. AP and scapular Y X-rays characterize most fractures. CT scan with 3D reconstruction guides surgical planning for displaced multi-part fractures. Axillary nerve and brachial plexus function must be documented.
Treatment Path
how care progresses at OSI1
Sling immobilization
For minimally displaced and angulated fractures — the majority of proximal humerus fractures. Pendulum exercises begin early; supervised physical therapy at 2–4 weeks.
Surgical Options at OSI
if non-operative care isn't enoughSignificantly displaced multi-part fractures in physiologically young, active patients and valgus-impacted four-part fractures in appropriate patients may benefit from surgery. The balance between fixation and replacement depends on fracture pattern, bone quality, and patient demands.
Providers Who Treat Proximal Humerus Fracture
sports-medicine team

David B. Templin, M.D.

Trent Twitero, M.D.
Further Reading
authoritative sourcesExternal patient-education references and related OSI pages for additional background: