Overview
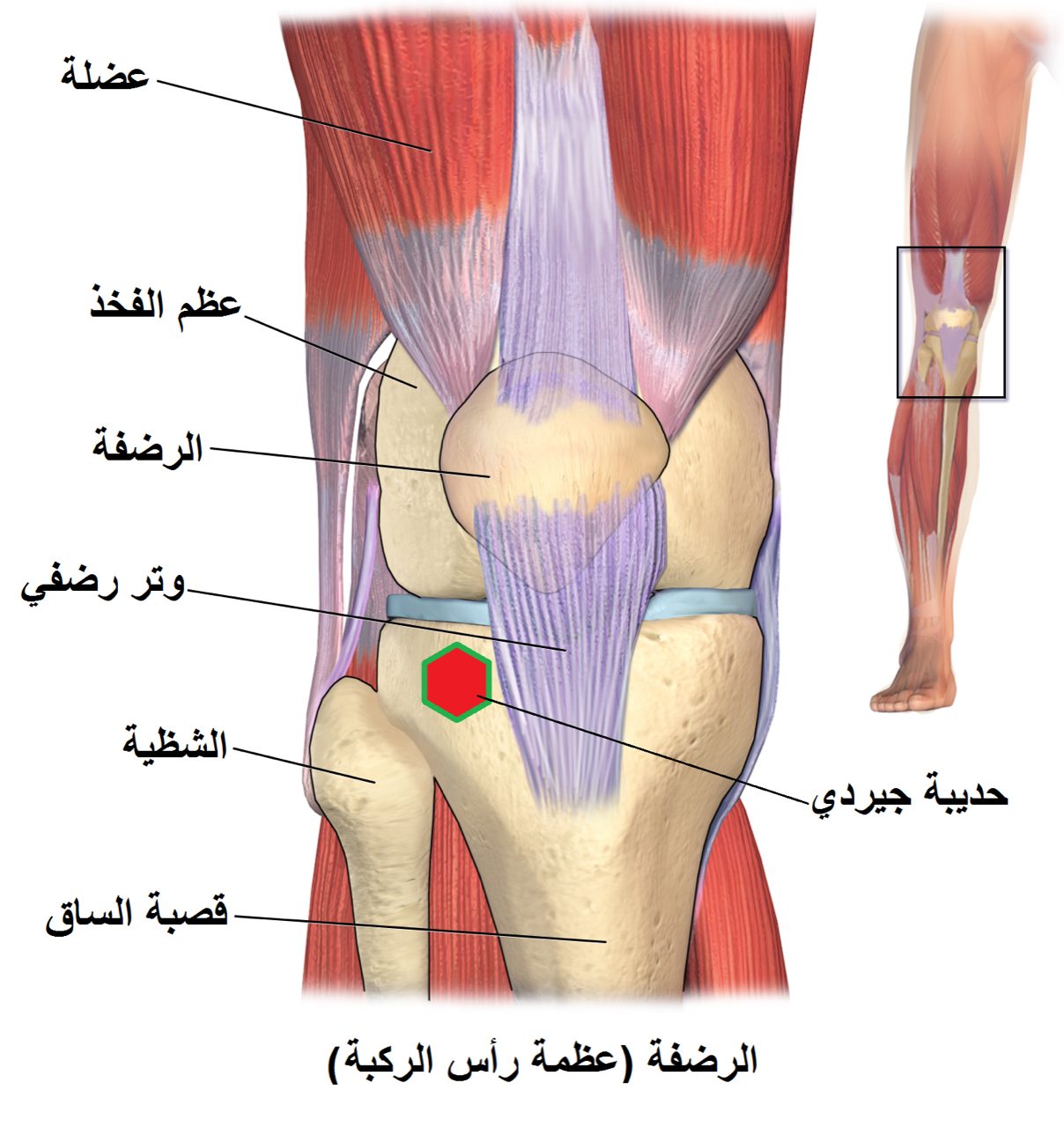
The knee has three compartments — medial, lateral, and patellofemoral. When arthritis affects only one, resurfacing the entire joint may be overkill. Partial knee replacement targets just the worn compartment and preserves the ACL, PCL, menisci, and healthy cartilage of the other two compartments. Patients often describe the result as feeling more like their own knee.
How the Procedure Works
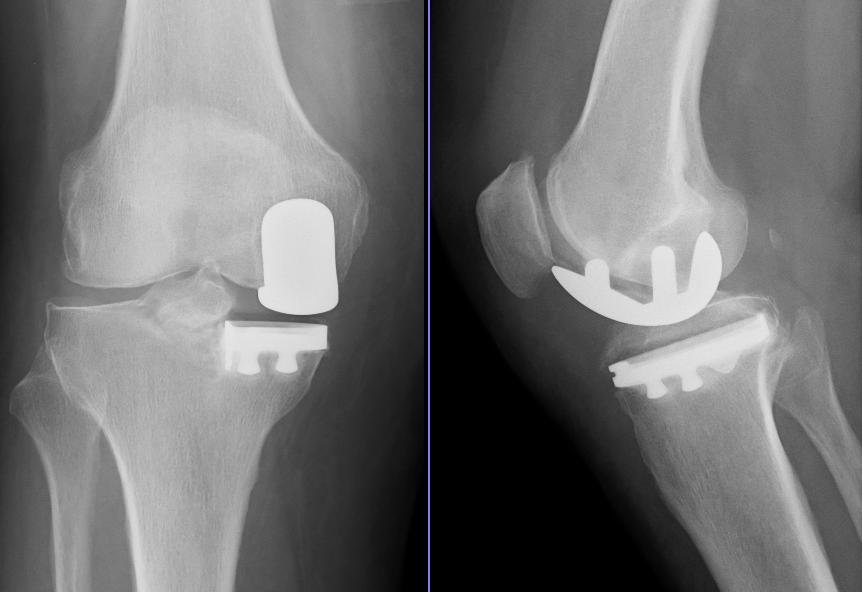
We resurface only the worn compartment — typically the medial femoral condyle and its matching tibial plateau — with a smaller metal-and-polyethylene implant. Both cruciate ligaments, the opposite compartment, and the patellofemoral joint are left entirely untouched. Patient selection is the most important factor in outcomes: the ACL must be functional (it drives the knee's natural rollback kinematics that a partial replacement relies on), the deformity must be passively correctable, and the other compartments must have intact cartilage. Implant sizing and tibial slope are set intraoperatively to match the native knee — the goal is a component that participates in normal knee motion rather than constraining it. The preserved ligament proprioception is why patients often describe partial replacement as feeling more like their own knee than a total replacement does.
When to Consider Partial (unicompartmental) Knee Replacement
Partial (unicompartmental) knee replacement is generally offered when symptoms, imaging, and a trial of non-operative care together point to surgery as the next step. The typical picture includes:
Single-compartment arthritis
Cartilage loss isolated to the medial or lateral compartment, confirmed on weight-bearing X-rays.
Intact ligaments
A functional ACL and PCL — the ligaments must still stabilize the knee for a partial replacement to work.
Correctable deformity
A varus or valgus deformity that reduces passively, suggesting the other compartments are still healthy.
Conditions This Treats
Physicians Who Perform Partial (unicompartmental) Knee Replacement


David B. Templin, M.D.

Trent Twitero, M.D.
Providers Who Surgically Assist with Partial (unicompartmental) Knee Replacement

Sydney Georg, PA-C
Ben Swanner, PA-C
Further Reading
External patient-education references and related OSI pages for additional background: