Overview
what it is and why it matters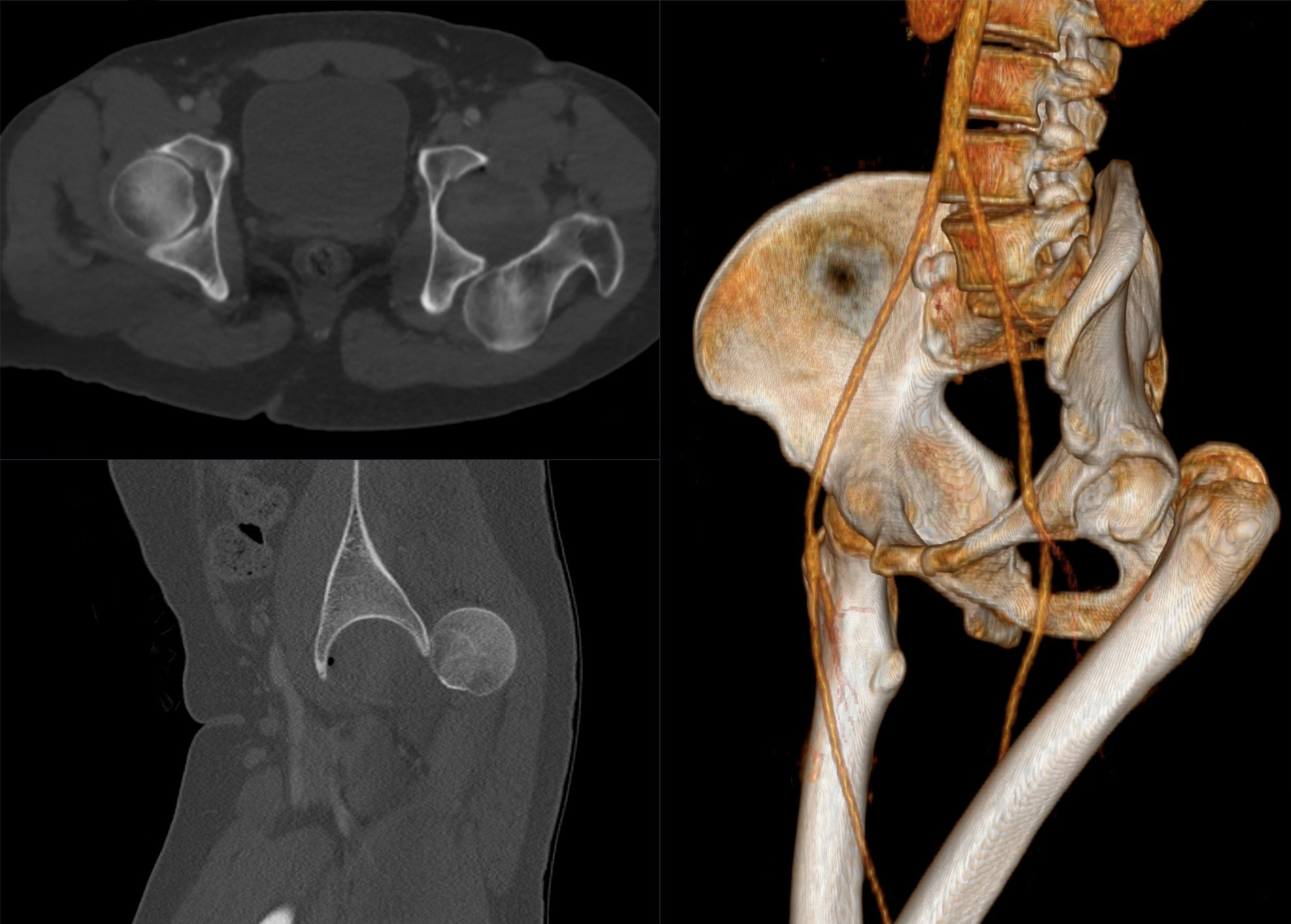
Hip dislocation occurs when the femoral head is forced out of the acetabulum. Posterior dislocation — where the hip is forced backward — accounts for approximately 90% of cases and typically results from high-energy impact such as a sports collision or fall from height. Anterior dislocation is less common and results from forced abduction and external rotation.
Hip dislocation is an emergency. The blood supply to the femoral head runs along the posterior capsule and is at risk with prolonged dislocation — avascular necrosis risk rises sharply after 6 hours. Associated femoral head, acetabular, or femoral neck fractures are present in up to 50% of cases.
Diagnosis
exam first, imaging secondPosterior dislocation presents with a shortened, internally rotated, and adducted leg. The patient is in severe pain. AP pelvis X-ray confirms the diagnosis. CT is mandatory after reduction to identify associated fractures and loose bodies. Sciatic nerve injury should be assessed — the nerve is at risk in posterior dislocations.
Treatment Path
how care progresses at OSI1
Closed reduction under sedation
Emergency closed reduction in the emergency department or operating room under adequate sedation and muscle relaxation — performed as soon as possible after injury to protect the femoral head blood supply.
2
Protected weight-bearing
After successful reduction and confirmation of stability, protected weight-bearing for 4–6 weeks.
Surgical Options at OSI
if non-operative care isn't enoughSurgery is required when closed reduction fails, when associated fractures require fixation, or when loose osteochondral fragments within the joint need removal.
Providers Who Treat Hip Dislocation
sports-medicine team

David B. Templin, M.D.

Trent Twitero, M.D.
Further Reading
authoritative sourcesExternal patient-education references and related OSI pages for additional background: