Overview
what it is and why it matters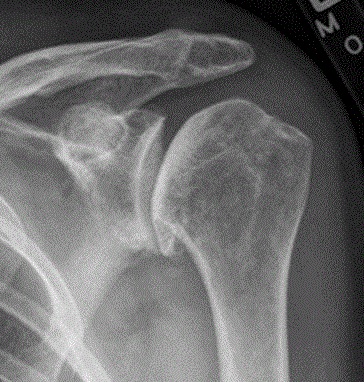
Shoulder osteoarthritis is the gradual wearing of the articular cartilage lining the glenohumeral joint — the ball-and-socket joint formed by the humeral head and the glenoid. It is less prevalent than hip or knee arthritis but causes significant pain and loss of motion. Primary (idiopathic) cases occur in older adults; secondary arthritis follows prior trauma, instability, rotator cuff tears, or inflammatory arthritis.
Posterior glenoid erosion — wearing down the back of the socket — is the characteristic pattern. This shifts the contact point of the ball posteriorly and worsens internal rotation loss.
Diagnosis
exam first, imaging secondDiffuse shoulder pain, progressive loss of internal rotation, and crepitus. Pain with passive rotation distinguishes glenohumeral arthritis from rotator cuff or acromial problems. X-rays show joint-space narrowing, subchondral sclerosis, and osteophytes. MRI evaluates glenoid bone loss, rotator cuff integrity, and fatty infiltration — critical for replacement planning.
Treatment Path
how care progresses at OSI1
Activity modification
Reducing heavy overhead loading and impact activities.
2
Physical therapy
Maintaining range of motion and strengthening the periscapular and rotator cuff muscles.
3
NSAIDs
Oral anti-inflammatories for symptom management.
Glenohumeral corticosteroid injection
Intra-articular injection — effective for short-term pain relief.
PRP or viscosupplementation
Options for patients wishing to delay surgery.
Surgical Options at OSI
if non-operative care isn't enoughProgressive arthritis that significantly limits daily activities and does not respond to conservative management is the main indication for shoulder replacement.
Providers Who Treat Shoulder Osteoarthritis
sports-medicine team

David B. Templin, M.D.

Trent Twitero, M.D.
Further Reading
authoritative sourcesExternal patient-education references and related OSI pages for additional background: